India has recorded notable progress in maternal and child health in the recent years. The state of Madhya Pradesh (MP), however, has performed sub-optimally compared to most states and union territories (UTs) of India. MP’s annual reduction in maternal mortality rate (MMR), for example, is at 5.8 percent, compared to the national average of 7.5 percent; the yearly drop in neonatal mortality rate (NMR) is at 0.6 percent, far below the national average of 3.8 percent. This report explores the key areas for intervention required to facilitate a more rapid reduction in MP’s maternal and child death rates. It identifies gaps in the areas of health and nutrition service delivery, human resources, governance, financing, data collection, and surveillance.
Attribution:
Ramesh Agarwal, et al., “Tracking India’s Path to Maternal and Child Health: A Case Study of Madhya Pradesh,” ORF Special Report No. 200, November 2022, Observer Research Foundation.
Introduction
In the past two decades, India has made significant strides in reducing maternal, newborn, and infant mortality. Progress has been uneven, however, and some states are performing significantly better than others. This special report examines the progress of Madhya Pradesh (MP) in improving these outcomes and achieving Goal-3 of the Sustainable Development Goals (SDGs), i.e., ‘Good Health and Well-being: To ensure healthy lives and promote well-being for all at all ages.’ Madhya Pradesh is one of India’s biggest states and is home to six percent of the country’s population. It has historically been saddled with difficult topography and continues to endure a host of economic and social challenges.
Although MP has scored improvements in the last 20 years,[1]it records the highest Neonatal Mortality Rate (NMR), Infant Mortality Rate (IMR), and Under-5 Mortality Rate (U5MR), and the third-highest Maternal Mortality Rate (MMR) among India’s larger states.[2],[3]
Table 1: Performance in Key Health Outcome Indicators (2014-2018)
Source:NITI Aayog State Heath Index Round 4, 2019-2020[4]
NITI Aayog’s SDG Index 2020-21[a],[5]classifies Madhya Pradesh as a ‘Performer’ state in SDG-3, among the bottom half of all states and union territories (UTs) (see Figure 1).
The SDG-3 index accounts not only for maternal and child health, but also for the following variables: Maternal Mortality Ratio (per 1,00,000 live births); Under-5 mortality rate (per 1,000 live births); Percentage of children in the age group 9-11 months fully immunised; Total case notification rate of Tuberculosis per 1,00,000 population; HIV incidence per 1,000 uninfected population; Suicide rate (per 1,00,000 population); Death rate due to road traffic accidents (per 1,00,000 population); Percentage of institutional deliveries out of the total deliveries reported; Monthly per capita out-of-pocket expenditure on health as a share of Monthly Per capita Consumption Expenditure (MPCE); and Total physicians, nurses and midwives per 10,000 population. This analysis focuses on the maternal and child health aspects of SDG-3.
I. Madhya Pradesh’s Successes and Failures
Earlier studies on Madhya Pradesh have evaluated the drivers of success in reducing IMR, MMR, and NMR using both qualitative and quantitative approaches. A 2021 study by India Health Action Trust (IHAT)[6]found that MMR and NMR have decreased in MP over the last 10 years. However, from 2012 to 2017, the annual rate of reduction for MMR in Madhya Pradesh was 5.8 percent, lower than the national reduction rate of 7.5 percent. The rate of reduction of NMR was 0.6 percent, significantly lower than the all-India reduction rate of 3.8 percent.[7]To meet the SDG 2030 targets of less than 70 maternal deaths per 100,000 live births and 12 neonatal deaths per 1,000 live births, Madhya Pradesh will need to accelerate the Annual Absolute Rate of Reduction (AARR) in MMR and NMR to 6.8 percent and 8.6 percent, respectively.[8]The same study found inter-district heterogeneity and proposed interventions such as improving antenatal care (ANC) and postnatal care (PNC) services, reducing home delivery, and increasing the availability of health facilities, particularly in the tribal districts.
Figure 1: Performance of States and UTs on SDG-3
Source:SDG India Index & Dashboard, 2020-21: Partnerships in The Decade of Action, NITI Aayog, 2020-21
A 2022 maternal and newborn health exemplar study[b],[9]that sought to observe the drivers of declines in maternal and newborn mortality, clustered the states and UTs of India into two broad categories: states with higher maternal and neonatal mortality and lower per capita income at baseline (2000), and states with lower maternal and neonatal mortality and higher per capita income at baseline. Madhya Pradesh was grouped in the first category, with Rajasthan, Orissa, Bihar, Jharkhand, Uttar Pradesh, Uttarakhand, Chhattisgarh, and Assam. In contrast to other High Mortality States (HMS), MP had an MMR that was found to be lower up until 2016, while the NMR was observed to be higher than the state cluster since 1985 (see Figure 2b).
Since the study, however, MP’s NMR has been decreasing, and the same pattern is seen in inter-district heterogeneity.[10],[11]The study concludes that while MP has made significant progress in reducing MMR, NMR, and IMR, it still lags behind other HMS. It recommends specific key priorities to further improve the state’s MMR, IMR, and NMR outcomes: targeted interventions in enhancing the quality of intrapartum and immediate postpartum care; addressing difficulties in reaching facilities; and mandating a minimum of 48 hours of stay in facilities.
Figures 2a and 2b: MMR and NMR Trends in Madhya Pradesh Vs. State Cluster and All-India (SRS 2019)[12]
Source:India: Maternal and Newborn Health Exemplar Study[13]
Figure 2a shows that between 2000 and 2019, MP reduced maternal mortality from 407 to 163 per 100,000 live births; neonatal mortality from 59 to 33 per 1,000 live births; infant mortality from 88 to 46 per 1,000 live births; and U-5 mortality from 110 to 53 per 1,000 live births. However, when compared to all-India averages and the outcomes for many other large states, MP has performed poorly. Better-performing states such as Tamil Nadu, Maharashtra, and West Bengal, have achieved better outcomes by increasing the coverage of effective interventions and focusing on the provision of high-quality care.
State government data shows that MP has been able to accelerate mortality rate reductions over the last two decades (see Figure 3). MP’s Annual Absolute Rate of Reduction (AARR) in this variable increased from 2.7 percent between 2000 and 2010, to 3.6 percent between 2011 and 2019.
Figure 3: NMR Trends and Projections for Madhya Pradesh (2000-2060)
Source:Report on Reducing MMR, IMR, and NMR in Madhya Pradesh, Task Force ON NMR, IMR, and MMR reduction in Madhya Pradesh, The General Administration Department, Govt. of Madhya Pradesh[14]
Even at this accelerated AARR, however, the state would only be able to meet the SDG target of single-digit NMR by 2055, rather than 2030. The required AARR, to meet the SDG target of single-digit NMR by 2030, is 16.2 percent beginning this year.
Various studies could help show the way to achieving the target. Toppo et al.,[15]for example, emphasise the importance of postpartum prudence. Their study found that the majority of deaths occurred in the postpartum period (postnatal deaths: 49 percent, antenatal deaths: 30 percent; and intranatal deaths: 20 percent). It blamed poor antenatal care and lack of human resources as leading causes of death in all the facilities considered by the authors.
For their part, Singh et al.[16]argue for prioritising districts with higher mortality rates as their analysis revealed inter-district heterogeneity. To reduce IMR, the study recommended full ANC, increased institutional delivery, routine postnatal checkups, full immunisation, and nutrition interventions. Meanwhile, Joshi et al.[17]make a case for providing pregnant women access to high-quality antenatal and postnatal care, and promoting healthy birth practices. The authors examined the impacts of maternal age, birth interval, and parity[c]on neonatal (NM), postnatal (PNM), and child mortality (CM). Children born to mothers between the ages of 20 and 30 were found to have the lowest NM, PNM, and CM. They also noted that short birth intervals and multipara (>3 children) contributed to a rise in MMR risk. The analysis found a correlation between MMR and low literacy and socioeconomic levels.
In January 2022, the Madhya Pradesh government established a high-level Task Force tasked to identify key areas for focused intervention over the next decade. The task force has conducted an assessment of the various stakeholders in the state’s health ecosystem to identify critical gaps and issues in service delivery, health resources, governance, nutrition interventions, financing, and data surveillance.[18]
A report released by the Task Force[19]outlined the issues affecting Madhya Pradesh’s maternal and child healthcare delivery system and proposed a framework that included building physical infrastructure, nurturing human resources, meeting the special healthcare needs of pregnant women and newborns, monitoring and surveillance of high-risk cases, improved health financing, and better governance.
II. Key Areas of Intervention
The report[20]underlines that if interventions are scaled up to 90-percent coverage and care quality is improved, up to 75 percent of maternal and neonatal mortality in low- and middle-income countries (LMICs) can be avoided. The India Newborn Action Plan (INAP), 2014[21]lays out a clear path to achieving single-digit NMR; for reducing MMR, the Ending Preventable Maternal Mortality (EPMM) is a similar document. INAP offers six packages to improve MNH care by focusing on the various stages of pregnancy and labour, and the neonatal period (see Figure 4).
Figure 4: Elements of INAP Framework for Reducing NMR
Source:Report on Reducing MMR, IMR, and NMR in Madhya Pradesh, Task Force ON NMR, IMR, and MMR reduction in Madhya Pradesh, The General Administration Department, Govt. of Madhya Pradesh
Improving Coverage and Quality of Care
Certain priorities exist that can be pursued by MP to reduce mortality. The state has not been able to scale up crucial interventions to levels greater than 90 percent. The quality of care provided and implementation has also been sub-par.
a. Coverage of key interventions and service quality
A pressing issue is the large number of pregnancies, births, and deaths that are unaccounted for.[22]From April 2021 to March 2022 a total of 1.2 million pregnancies and 1.3 million births were reported, compared to a projected total of 2.05 million births. Moreover, only 26 percent of estimated U-5 deaths are reported.
The lack of functional SNCUs and the low nurses-to-babies ratio at the state’s SNCUs must also be given attention. The current nurse-to-baby ratio of 1:5 to 7 must be increased to 1:2 in accordance with Staff Inspection Unit (SIU) guidelines. All of these factors contribute to low SNCU discharge rates (79.5 percent in 2021), compared to more than 90 percent in a high‐performing state like Tamil Nadu. SNCUs in MP can potentially reduce NMR by 5 percentage points by addressing human resource gaps.
The report also emphasises the gaps in emergency service implementation. Only about 31 percent of all calls received were classified as emergency, with more than 30 percent not even being served. The response time delay also contributes to poor quality of service, with delays ranging from 25 minutes in urban areas to 28 minutes in rural areas. This is exacerbated by the shortage of Advanced Life Support System ambulances, resulting in only 17 percent receiving pre-hospital medical treatment. Limitations were also apparent in the training of On Skill Birth Attendants (SBAs):[23]the task force found that the officers of the training programmes were mostly gynaecologists who were already overburdened with clinical and administrative duties.
b. The improvement framework
The task force determined that 75 percent of maternal deaths, stillbirths, and neonatal deaths in the state occurred during childbirth and the early neonatal period. It stressed that NMR will be the most important indicator to monitor in the years ahead.
Table 2: Phases in Implementation of Interventions in Maternal and Newborn Health
The following areas require intense focus in the short term:
Improving care around childbirth and the infant’s first week of life: Evidence suggests that providing high-quality care during the intrapartum period and at birth, including optimum resuscitation and care of sick and small newborns, can reduce mortality by 50 to 60 percent.
Monitoring high-risk pregnancies from conception, providing antenatal care, and assisting with delivery in Sub-District/Sub-Divisional Hospitals (SDH) and District Hospitals (DH) can also yield benefits. In high-risk pregnancies, determining correct gestation via first trimester ultrasound is critical for the timely prescription of antenatal corticosteroids if the mother goes into pre-term labour.
Filling Gaps in Health Resources
Restructuring the health sector’s resources will be crucial to achieving MP’s objectives and SDG-3. This encompasses community involvement, telemedicine, physical infrastructure, drugs, medical equipment, referral transport services, and public healthcare delivery services.
a. Inter-District Heterogeneity
The task force report[24]noted the district-wide variations in deliveries attended by SBAs, based on the fifth round of the National Family Health Survey.[25]It called for particular attention to the districts of Singroli, Sidhi, and Rewa in terms of postnatal care.
Figure 5: Births Attended by SBAs and Children Who Received Postnatal Care from Medical Personnel (2020-21)
Source:NFHS 5 (2019-21)[26] Note:They received postnatal care from a medical professional within 2 days of delivery.
Findings of the NFHS-5 show a direct link between children who received postpartum care within two days of delivery and deliveries attended by trained medical staff. In Figure 5, the data reveals a notable variation between the districts of MP. In districts such as Indore, Neemuch, and Dhar, a high proportion of births (95 percent) are attended by trained healthcare professionals, and a high percentage of infants (90 percent) receive postnatal treatment from trained healthcare professionals within two days of birth. Meanwhile, in areas like Singroli, Narmadapuram, and Sheopur, less than 85 percent of deliveries are attended by trained medical professionals, and less than 75 percent of infants receive postnatal care within two days of birth.
b. Infrastructure
According to the Rural Health Statistics Report 2020-21,[27]there are 10,189 Sub Health Centers, Primary Health Centers 1,518 (1,234 Rural and 284 Urban), Community Health Centers 320 (Rural-295 and Urban-25), 92 Sub-district Hospitals, 51 Districts Hospitals, and 10 Medical Colleges in the state. Table 3 summarises the population coverage of the state’s rural health infrastructure, and the all-India average.
Table 3: Coverage of Rural Health Infrastructure in Madhya Pradesh (as of 31 March 2021)
Source:Rural Health Statistics, Ministry of Health and Family Welfare 2020-21
c. Human Resources
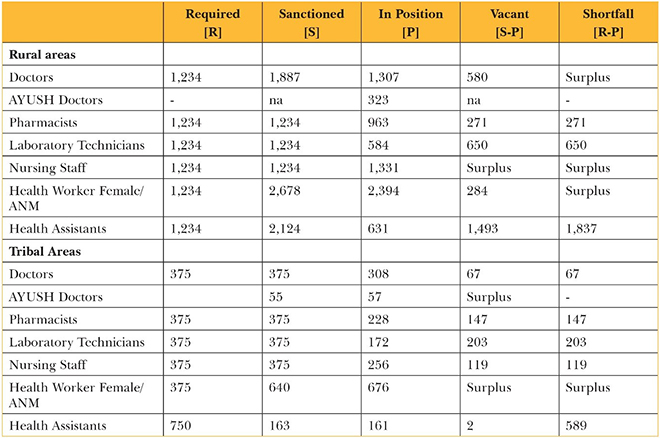
The shortfall in specialist, medical, and paramedical staff is more acute in remote regions. Tables 4 and 5 give a snapshot of the state of human resource strength in Madhya Pradesh.
Table 4: Human Resources at SHCs in Madhya Pradesh (as of 31 March 2021)
Source:Rural Health Statistics, Ministry of Health and Family Welfare 2020-21
Table 5: Human Resources at PHCs in Madhya Pradesh (as of 31 March 2021)
Source:Rural Health Statistics, Ministry of Health and Family Welfare 2020-21
Focus on Nutrition
Malnutrition is an important factor for high MMR, NMR and IMR,[28]and 68 percent of all child deaths in India are attributed to malnutrition.[29]According to the most recent Comprehensive National Nutrition Survey (CNNS) 2019, 32 percent of children and adolescents aged 10 to 19 in MP are moderate to severely thin. Micronutrient deficiency, or ‘hidden hunger’, affects 28.7 percent of girls (10-19 years) in the form of anaemia, 74.5 percent in folate deficiency, and 23 percent in Vitamin D deficiency in girls and boys (10-19 years).[30]
At the same time, stunting—which indicates chronic malnutrition—decreased by 6.3 percentage points in the five years between NFHS-4 and the fifth round; exhaustion, which indicates acute malnutrition, has gone down by 6.8 percentage points in the same period. At 9.8 percent, the proportion of low-birth-weight infants—which indicates both acute and chronic malnutrition—has recorded the biggest reduction. The prevalence of underweight in women also fell from 28.4 percent in NFHS-4 to 23 percent in NFHS-5.
However, as in other parts of India, anaemia remains prevalent due to micronutrient deficiency. Anaemia has increased from 68.9 percent (NFHS-4) to 72.7 percent (NFHS-5) in children aged 6 to 59 months across the state. Young children’s complementary eating habits have deteriorated during this period. The state’s essential nutrition-specific and sensitive service indicators, such as antenatal care, early initiation of breastfeeding, exclusive breastfeeding, iron and folic acid supplementation, vitamin A supplementation, and immunisation, have also improved between the two latest rounds of NFHS.
The task force report utilises UNICEF’s Conceptual Framework for Determinants of Undernutrition to evaluate the nutritional scenario in the state and the pathways by which nutrition affects MMR, IMR, and RMN. The framework depicts the levels of undernourishment indicators in women and children, classified as immediate, fundamental, or permissive. The study identified new initiatives and interventions that may fill gaps in the current delivery model.
Figure 6: Nutrition Pathways to Reduce NMR, IMR and MMR in Madhya Pradesh
Source:Report on Reducing MMR, IMR, and NMR in Madhya Pradesh, Task Force ON NMR, IMR, and MMR reduction in Madhya Pradesh, The General Administration Department, Govt. of Madhya Pradesh
III. Health Data Surveillance
Health data surveillance remains a significant challenge for MP.[31]For example, the authors of this report compared the estimated infant mortality based on precision-weighted estimates of neonatal, post-neonatal, and child mortality for 640 districts in India, NFHS 2016,[32]and the registered deaths in the Civil Registration System (CRS), 2019 and found a significant difference between registered deaths and estimated infant mortality across the state’s districts. The mean percentage difference in infant mortality observed across all districts was 160.2, with a standard deviation of 35.4.[d]This significant discrepancy is an indication that the CRS is not accurately recording many deaths.
MP should mitigate this challenge, given that it had the nation’s highest rate of infant fatalities in 2019–20.[33]For instance, Burhanpur district reported zero infant deaths in the CRS 2019,[34]yet, the precision-weighted infant mortality for the district is 48.4.[35]The districts of Burhanpur, Alirajpur, Sidhi, Raisen, Barwani, Mandsaur, Umariya, Chhatarpur, Bhind, and Morena had the greatest divergence in the registered and project deaths and need active monitoring.
Gaps in State Data Tracking System
Targeted assistance is required in Madhya Pradesh for community-level data gathering. Only six of the 51 districts had more registered pregnancies than deliveries. This suggests that either the system is slow to update the data or that end-users (Auxiliary Nurse Midwifes or ANMs, and Data Entry Operators or DEOs) are not uploading the data in a timely manner. Discrepancies between the estimated neonatal mortality and the recorded neonatal deaths still exist despite the introduction of the ANMOL platform. With a standard deviation of 18.9, the mean percentage difference across all districts is 174.4. In the districts, an average of 397 HRPW are found for every 1,000 pregnant women who are enrolled. Similarly, for every 1,000 deliveries, a problem occurs during delivery in about 373 occasions. The task force also noted that more claims for delivery benefits than ANC benefits are completed, which suggests that ANC information in the HMIS platform are not updated in real time. (see Figure 7).
Figure 7: Delivery Benefits Claimed Vs. ANC Benefits Claimed: Negative Correlation Found
Data Source:Anmol RCH Portal, NHM compiled Report on DBT
Figures 8a and 8b: Precision-weighted Estimated INMR Vs. Registered Infant and Neonatal Deaths, Madhya Pradesh Districts
Data Sources:Estimated IMR: Precision-weighted estimates of neonatal, post-neonatal and child mortality for 640 districts in India, NFHS 2016 Registered Deaths:Vital statistics of India based on the Civil Registration System, 2019
The task force identified crucial concerns that need to be addressed in upcoming versions of the ANMOL platform to improve the data quality:
Block Program Managers (BPMs) and DEOs at the healthcare institutions confirmed ANMs’ reports of delays in data synchronisation between handheld applications and the online portal. The typical waiting period ranges from three to four days.
Pregnant women cannot register in the ANMOL database with the app unless they have a Samagra[36]ID and a bank account. This is a particular problem for significant populations, such as migrant workers.
The pregnancy outcome of the pregnant woman is not displayed by the ANM ANMOL app.
To eliminate beneficiary payment delays, the PFMS platform, which was integrated with ANMOL, does not accept submissions from minor payment banks whose IFSC codes are not registered with the system. The application also rejects several banks with updated IFSC codes, such FINO Bank.
Inaccurate block mapping for ANMs in the ANMOL app.
Insufficient training for ANMs to use the app properly, especially for new features after an app update.
A lack of suitable notifications for debugging failures and an error code manual within the app.
The limited alternatives for correcting information that was entered improperly during registration.
Lack of an app support system that will allow users to voice complaints directly via the app.
Administrative issues: Delays in Samagra[37]validation, delays in Public Finance Management System (PFMS)[38]validation in financial management systems, and inaccurate and incomplete end-user input.
Two ways to reduce cross-platform synchronisation problems are monitoring data pipeline synchronisation jobs on a frequent basis and sending potential delay notifications and confirmation notifications to end-users as soon as synchronisation is finished. The ANM block dictionary can be updated to quickly change ANM block mappings from the back-end.
Figure 9: TeCHO+ Data Quality Assurance Module
Source:Report on Reducing MMR, IMR, and NMR in Madhya Pradesh, Task Force ON NMR, IMR, and MMR reduction in Madhya Pradesh, The General Administration Department, Govt. of Madhya Pradesh
The report also emphasises that not enough training programmes are being made available to end-users. It recommends that MP draw lessons from Gujarat’s TeCHO+ platform,[e]which implemented a training module followed by a certification option. As a follow-up, ANMOL could put in place a ticketing system with a special group of people to handle app support, letting users report unusual behaviour or issues with the programme. To enhance the accuracy and timeliness of the data, another option is to use the independent data validation and verification system (shown in Gujarat in Fig. 9).
Data availability is critical for monitoring and validation purposes. ANC and HRPW data are currently only available in line list format.[f]Aside from the current indicators, aggregated data on four ANC check-ups per 1,000 pregnant women, as well as the Direct Benefit Transfer (DBT) claim settlement rate, are desirable at the block level.
IV. Challenges in Financing
Public health insurance continues to be the main source of funding for healthcare in India.[39]While the Ayushman Bharat Pradhan Mantri Jan Arogya Yojana’s (AB PM-JAY) has had some degree of success, the system continues to show gaps that force participants to spend out-of-pocket for medical care. Despite recent declines in out-of-pocket expenses (OOPE) as percentage of health spending, India continues to be among the developing nations with the highest figures in this variable. Targeted financing and prepayments plans are needed to reduce out-of-pocket costs and move closer to affordable healthcare.
Innovative Health Financing Instruments
a. Family Health Account: Madhya Pradesh has enhanced access to secondary and tertiary care services through the Deen Dayal Swasthya Suraksha Parishad’s Ayushman Bharat-Madhya Pradesh Niramayam Yojana. Primary care must be made accessible, though, as it is a significant contributor to high OOPE. Supporting primary care financially will have three positive effects: relieve beneficiaries of the financial burden of OOPE for availing primary healthcare, decrease the burden of primary care treatment on district hospitals and medical colleges, and provide scope to improve quality of care at district hospitals and medical colleges by reducing overcrowding.
The task force proposes the creation of a Family Health Account as part of the Ayushman Bharat Digital Mission (AB DM). The proposal includes a fixed amount of assured sum in the beneficiaries’ family health cards, entitling them to cashless treatment at accredited facilities. This approach will provide beneficiaries with different pathways for access to primary care, eventually reducing the burden on public hospitals and, in turn, ensuring an equitable distribution of patient load across facilities.
Current evidence shows that increasing financial support for Outpatient Department (OPD) results in a significant reduction in Inpatient Department (IPD) expenses as well as the duration of hospitalisation. This reduces the strain on hospitals and the state’s limited tertiary care capacity.
b. Health Outcome Fund: Another tool for targeted interventions is a health outcome fund geared towards maternal and child healthcare. The distribution of funds is contingent on the achievement of specific objectives. Outcome funds are increasingly being considered as a means to scale up outcome-based contracts and impact bonds, thereby increasing the value of funding, the number of contracts and stakeholders reached, and the number of service users served. In Rajasthan, such impact bonds have proven to be effective.[40],[41]
Aiming for economic efficiency by shifting funds from ineffective projects to those with demonstrable, verifiable effects, is a rationale for using outcomes funds. They can also accelerate learning about innovation interventions and/or outcomes-based funding itself.
V. Weaknesses in Governance
Madhya Pradesh must scale-up key interventions to 90-percent or higher coverage and improve care quality. A system of regular reviews at all levels is required to detect and close gaps between authorities in a reasonable timeframe, in addition to immediate external facilitation. The state’s current review mechanism is infrequent and inefficient. The task force report[42]recommends periodic and timely reviews as a means of strengthening governance and making healthcare a priority for the state.
The following steps are proposed for this purpose:
Mechanism of audit and identification of gaps at all levels; efficient and effective closure of these gaps would be a key strategy.
Monthly review by Chief Minister of key health parameters and outcomes.
Identifying issues in governance and accountability not only of health functionaries but also administrative personnel.
An internal review at all levels by the facility in charge, Chief Medical Officer (CMO), District Collector and Mission Director, National Health Mission (MD, NHM). Joint meetings with concerned departments would be a platform to resolve issues.
Identifying parameters to be monitored: structure, process, and patient-centric outcomes.
Using existing policies and tools (INAP, IPHS standards, LaQshya, SUMAN, MUSKKAN, SAMPARK, SAMAGRA) to assess the effectiveness of facilities and services.
Bridging gaps in a time-bound manner. These gaps are likely to be diverse in the domains of structure, process, and outcomes.
Providing adequate resources effectively and efficiently, from the state or through other means.
Clearing inefficiencies in the system and eliminating wasteful care.
Instituting mechanisms to enhance the skills of the providers (skills laboratories, self-learning modules) and the capacity of the facilities to undertake Qi exercises. Appropriate reward mechanisms are instituted.
Instituting a strong logistic management information system for all supplies under Health and WCD.
Promoting community engagement and identifying human resources among adolescents and youth and nurturing them as change agents.
External monitoring and evaluation
Constituting an external expert group (Health Steering Committee) to focus of monitoring and evaluation. This group performs external random audits and monitors the program and the closure of gaps identified in the review meetings. It provides feedback to state health functionaries.
The committee participates in a subset of review meetings and monitors the quality of the reviews; it regularly participates in the CM review; and it dispenses advice on emerging evidence and experiences that worked in other states and countries
Review Mechanism
The state’s current review procedure is inconsistent and ineffectual. While there is a review procedure at the levels of the District Collector, MD NHM, and Chief Minister, there is a need to establish specific goals at the block and facility levels to concentrate on areas that need development.
A multifaceted strategy is required to effect an overhaul in the maternal and child health situation in Madhya Pradesh. Such a strategy should focus on interventions not only in the health sector, but also in non-health initiatives including nutrition, water and sanitation, gender inequities, and other social issues such as female foeticide and contraceptive awareness and use. The public health system will play a crucial role in enhancing the overall RMNCH+A condition. The private sector plays a significant and expanding role, but it cannot take the place of publicly funded, high-quality healthcare that is easily accessible and reasonably priced. Therefore, it would be crucial to strengthen the public health sector in terms of suitable infrastructure, the availability of qualified and dedicated human resources, ensuring that the providers are adequately skilled and responsive, and that there is constant funding flow. Increasing healthcare capacity, rewarding and recognising employees, and forming public-private partnerships are other complementary strategies that can be tested and thereafter scaled up.
According to the National Healthcare Resource Repository’s 2019 Healthcare Census of India, there are 66,208 health facilities in MP, of which 13,595 (20 percent) are public and the remaining 52,613 (80 percent) are private. Figure 10 illustrates how more than half (55 percent) of the poor (bottom 40 percent) rely mostly on the private sector to meet their requirements (NFHS4).[43]Therefore, the private sector must engage with government initiatives to enhance health outcomes; a regulatory framework will need to be created for the same.
Figure 10: Where Do the Poor Go for Healthcare?
Source:Report on Reducing MMR, IMR, and NMR in Madhya Pradesh, Task Force ON NMR, IMR, and MMR reduction in Madhya Pradesh, The General Administration Department, Govt. of Madhya Pradesh
Public-Private Partnership (PPP) models are widely used, including in MP-JAY. This should be strengthened by including them in public data platforms such as ANMOL and others where a large number of deliveries occur. Experimentation with training, mentoring modules, and other aspects should be encouraged.
This present report recommends that the state of MP involve development partners and civil society[g]in this widespread effort aimed at MMR, NMR, and IMR. Philanthropies can generate resources and contribute a wealth of technical know-how and human resources.
Conclusion
Over the recent years, Madhya Pradesh has recorded significant progress in reducing maternal, neonatal, and infant mortality. However, the state has a long way to go before it can meet the SDG-3 target of health and well-being for all. This report analysed various studies on the state of maternal and child health in Madhya Pradesh to cull the most important challenges.
The report highlighted specific interventions in areas encompassing delivery of health services, health resources, governance, nutrition, financing, and data infrastructure. An imperative is to seek convergence between the different segments of the health and other relevant government departments. The introduction of client education about reproductive, maternal, newborn, child, and adolescent health (RMNCH+A) can help MP. The state can take advantage of a decentralised and democratic approach to real-time health interventions by utilising the Crisis Management Committee set up during the COVID-19 pandemic and the Laadli Laxmi Scheme to prepare the future cohort for RMNCH+A interventions.
Ramesh Agarwalis Associate Professor, WHO Collaborating Centre for Training and Research in Newborn Care, All India Institute of Medical Sciences.
Sikim Chakrabortyis Associate Fellow for Data Sciences at ORF.
Suparna Ghosh-Jerathis Program Head for Nutrition at The George Institute for Global Health India.
Shamika Raviis Vice President for Economic Policy at ORF.
Endnotes
[a]Since 2018, NITI Aayog’s SDG Index has been providing aggregate assessments of India’s progress towards SDG-2030 at a sub-national level. Based on their performance across the 16 SDGs, the states and UTs are grouped into four categories: Aspirant (0-49), Performer (50-64), Front Runner (65-99), and Achiever (100).
[b]The exemplar methodology draws on a mixed-methods approach to identify the drivers of change, dividing the interrelated factors hierarchically in distal, intermediate and proximate drivers of maternal and neonatal mortality decline. India, Bangladesh, Ethiopia, Morocco, Nepal, Niger, and Sengal are the seven countries included in this global maternal and newborn health exemplar study. It was a collaborative effort by the International Institute for Population Sciences (IIPS), the National Health Systems Resource Centre (NHSRC), the India Health Action Trust (IHAT), and the University of Manitoba.
[c]‘Parity’ is the number of times a woman has given birth to a live neonate (any gestation) at >=6months/24 weeks, regardless of it was a livebirth or stillbirth.
[d]The standard deviation indicates that the differences range from 125% to 195% (very high across all the districts) and the mean difference is not a heavily skewed number.
[e]Gujarat’s TeCHO+ State of Health is a real-time integrated health surveillance platform that has been operational since April 2019.
[g]These can include institutions such as Tata Trusts Piramal Foundation, and MSD for Mothers that have extensive experience in these areas.
[9]India: Maternal and Newborn Health Exemplar Study, National Health Systems Resource Centre, International Institute for Population Sciences, India Health Action Trust, University of Manitoba, and Countdown to 2030 for Women’s, Children’s and Adolescents’ Health
[10]India: Maternal and Newborn Health Exemplar Study
[11]Institute for Health Metrics and Evaluation (IHME). Findings from the Global Burden of Disease Study, 2017. Seattle, WA: IHME, 2018.
[13]India: Maternal and Newborn Health Exemplar Study
[14]Task Force Report on Reducing MMR, IMR, and NMR in Madhya Pradesh
[15]Manju Toppo, Dinesh Kumar Pal, Devendra Gour, Veena Melwani, Amreen Khan, and Soumitra Sethia Addressing maternal mortality in selected Districts of Madhya Pradesh, India – A human rights-based approach. Indian J Community Med 2019;44:13841
[16]Singh P, John S. Determinants affecting infant and maternal mortality in Madhya Pradesh. Int J Health Sci Res. 2017; 7(11):176-184
[17]Krishna Prakash Joshi and S. S. Kushwah. “AN EPIDEMIOLOGICAL STUDY OF SOCIAL FACTORS ASSOCIATED WITH MATERNAL MORTALITY IN A COMMUNITY DEVELOPMENT BLOCK OF MADHYA
PRADESH.” Indian Journal of Community Health 23 (2011): 78-80.
[18]Report on Reducing MMR, IMR, and NMR in Madhya Pradesh, Task Force ON NMR, IMR, and MMR reduction in Madhya Pradesh, The General Administration Department, Govt. of Madhya Pradesh
[19]Task Force Report on Reducing MMR, IMR, and NMR
[23]Bali, Surya & Reddy, Venkatshiva. (2018). Evaluation of Competency and Skills of Skilled Birth Attendants in Madhya Pradesh, Central India. Indian Journal of Public Health. 62. 61-64. 10.4103/ijph.IJPH 332 16
[29]Rakhi Dandona et. al.. (2020). Subnational mapping of under-5 and neonatal mortality trends in India: the global burden of disease study 2000–17. The Lancet, 395(10237), 1640-1658.
[30]Ministry of Health and Family Welfare (MoHFW), Government of India, UNICEF and Population Council Comprehensive National Nutrition Survey (CNNS) National Report, 2019.
[32]Rockli Kim, Lathan Liou, Yun Xu, Rakesh Kumar, George Leckie, Mudit Kapoor, R Venkataramanan, Alok Kumar, William Joe, and S V Subramanian, Precision-weighted estimates of neonatal, post-neonatal and child mortality for 640 districts in India, National Family Health Survey 2016. Journal of global health, 10(2), 020405.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

 PDF Download
PDF Download