High-density urban agglomerations may be sustainable in terms of the economies of scale their populations provide. Yet, as proven by the ongoing COVID-19 pandemic, these same urban spaces are nearly defenceless in times of unprecedented disease outbreaks. A pandemic poses many risks to the millions who live in dense megacities, whether in wealthy countries or developing ones. The sheer density of the population of these cities provides an ideal environment for infections to erupt, and fast. This paper studies the densification of New York and London, both megacities, and how COVID-19 has virtually crippled their public health systems. It argues that India’s megacities can follow a similar trajectory if the ongoing countrywide lockdown fails to arrest the spread of the disease. The paper aims to assist Indian policymakers in working towards an optimal population density for the country’s urban agglomerations, and in developing a disaster response strategy for these megacities beyond the current pandemic.
Attribution:
Dhaval D Desai, “Urban Densities and the Covid-19 Pandemic: Upending the Sustainability Myth of Global Megacities,” ORF Occasional Paper No. 244, May 2020, Observer Research Foundation.
Introduction
Urban planners hold the view that denser city populations contribute to lowering the carbon footprints of these urban areas.[1]Densities facilitate the efficient use of scarce resources and services as they get distributed to a large number of people in shorter periods of time. Designed for use by millions of people, capital-intensive mega public projects make economic sense and reflect relatively low ‘per unit’ cost. For example, cities may contribute significantly to overall carbon dioxide emissions, but they are highly efficient in terms of per-capita emissions of greenhouse gases. Research has shown that higher population densities lead to less use of personal vehicles, more walking, more public transport options, and more energy-efficient homes and offices.
At the same time, however, high population densities also mean more vulnerabilities during a pandemic.
The rapid spread of the COVID-19 virus and the high death rates seen in hyperdense megacities across the world[2]should be a wakeup call for urban planners, designers, policymakers and administrators to reconsider the long-held belief thatdensercities are indeedbettercities. It is time to rethink how the overall ‘sustainability’ quotient of densities becomes not just counterproductive but also life-threatening in the face of biological disasters of the scale and magnitude of COVID-19.
A report published inForbesin March 2020, when the impact of the pandemic was just beginning to be felt across the world, highlighted data comparing population-adjusted COVID-19 cases in the 10 most-affected countries at that time.[3]The numbers of confirmed COVID-19 cases were compared with the numbers of confirmed cases adjusted to the population in China, the UK, the US, South Korea, France, Germany, Iran, Spain, Switzerland and Italy—from the time each country recorded one confirmed COVID-19 case per million population.
While adjusting for population showed the “relative strain” on a country, the “growth of the virus should be independent” of the size of the country, other factors being equal. However, since the quality of life and economic indicators differ across countries, “the raw numbers of cases are more telling on the current situation of a country”. In the countries surveyed—and their large metropolitan areas that are seeing a rapid increase in community-level infections, such as New York City and London—factors such as population density, quarantining, and strict adherence to social distancing play a much larger role in how the virus spreads than the size of the total population.
Over half of the world’s population—55 percent—live in cities, with the figure expected to rise to 68 percent by 2050.[4]Only a handful of countries will largely propel this growth. India and China in Asia, and Nigeria in Africa are expected to contribute the highest proportions to this rapid urbanisation, cumulatively accounting for about 35 percent of the world’s rural to urban transition between 2018 and 2050.[5]Currently, North America (82 percent), Latin America and the Caribbean (81 percent), and Europe (78 percent) account for most of the world’s urbanised regions, while Africa remains the most rural.[6]However, Africa faces a high risk of rapid transmission of diseases since many of its countries are also home to some of the world’s densest slum settlements. Sub-Saharan Africa, for instance, has the world’s highest percentage of urban population living in slums (62 percent).[7]
For South Asia, and particularly India, where large urban populations continue to live in poverty, it is important to understand the causes for the rapid spread of COVID-19.
Countries around the world are busy tackling the pandemic to curtail infection spread and fatalities, even as they try to strike a balance between saving lives and economic revival. As the number of cases soars, it has become increasingly clear that the predominance of COVID-19 has been in dense urban centres.[8]Mumbai, Milan, Madrid, London and New York City, all hyperdense global megacities, have accounted for the maximum number of COVID-19 cases and resultant deaths in their countries.
With there being no sign yet of a COVID-19 vaccine that will work, the coming weeks will be critical for the millions living in urban agglomerations around the world. The Indian government has imposed a nationwide lockdown to control the spread of the virus. In the absence of a vaccine, disciplined adherence to social distancing and similar measures are the only reliable methods to prevent the situation from quickly worsening in Mumbai and other urban agglomerations.[9]
However, with nearly 93 percent of its workforce engaged in the informal sector, and a sizeable number of those subsisting on daily wages, India’s 1.3 billion people face a quagmire, especially if the lockdown continues for a prolonged period. Already, India is witnessing reverse migration, as thousands of migrant workers, deprived of their means of survival in cities because of the lockdown, have begun returning to their villages.[10]Such a trend raises the prospect of the infection spreading to rural areas, where public health infrastructure is even more inadequate than that in cities.
Unrestrained population densities in urban sprawls put severe pressure on public resources and services. They also undermine and overwhelm public health systems during medical crises such as COVID-19, especially during the community-spread stage.
Indeed, the pandemic has exposed the frailties of even those global cities that boast of highly advanced medical and public health systems, mere weeks after the first cases were reported in those regions. With some of the world’s highest urban population densities and comparatively inadequate health facilities in its cities, India may have only seen the tip of the iceberg of the potential COVID-19 outbreak thus far.[11]
Vulnerable Cities: Case Studies
Unlike pandemics of the past, COVID-19 has the propensity to spread among human populations at a frenetic pace.[12]Since the initial outbreak of the virus in China’s Wuhan in December 2019, it took only a few weeks for multiple countries to be hit by the disease. In the absence of a reliable cure, it took hundreds of deaths for countries to realise that the only way to counter the threat was by restricting the movement of people and trade. As the intensive screening of international passengers and contact tracing proved to be a weak strategy, international airports and seaports were shut and land borders sealed. Several countries resorted to lockdowns of varying degrees to ensure that people stayed at home, minimising the spread of the infections. Social distancing and home isolation and home quarantine became the norm. Large cities with mega population densities proved to be particularly helpless, their well-established medical infrastructure paralysed in the face of mounting infections.
Why have several megacities been among the worst hit by the pandemic? To understand this, one only need to look at New York City and London. Often hailed as the global centres of wealth creation, both cities have also featured high on global urban sustainability rankings.[13]Both New York City and London have also shown a remarkable similarity in not just registering the highest number of COVID-19 cases in the US and UK respectively, but also the highest number of fatalities in those countries.
New York City
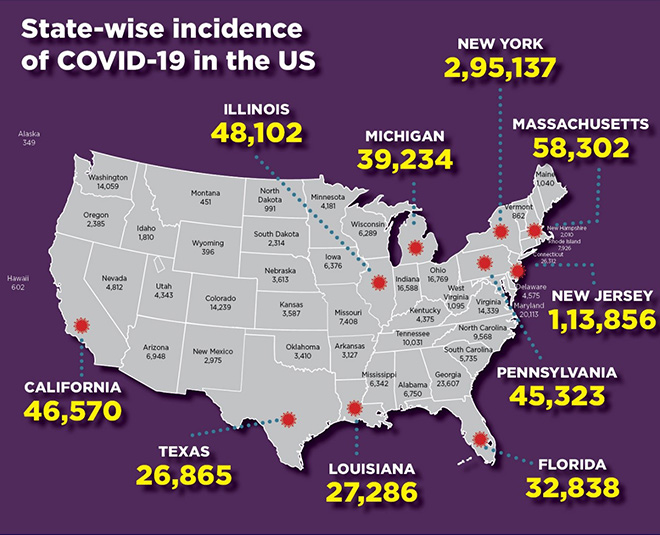
As of 27 April 2020, the US has over 987,691 confirmed COVID-19 cases, nearly 292,027 of which have been identified in New York City alone.[14]With 17,000-plus deaths, New York City also leads in the US’ COVID-19 mortality rate.
When a small number of cases were first identified in the New York City suburb of New Rochelle, local and state officials swung into action to contain the outbreak. The National Guard was deployed,[15]and the health workers started contact-tracing of the patients. With increased testing, hundreds of new confirmed cases emerged from all five New York City boroughs and the number of deaths began to surge. The state administration eventually ordered the closure of schools and businesses, sought the help of retired doctors and medical professionals to supplement the human capital already deployed to contain the virus[16]and sent an SOS to the federal government in Washington DC to ramp up hospital equipment. Manhattan’s Jacob K Javits Convention Center was converted into a makeshift hospital with the help of the US army.[17]However, at a time when social distancing was an absolute inevitability, the Donald Trump-led federal administration preferred to safeguard the economy over human lives.[18]The failure to impose strict lockdowns allowed a fair degree of free economic activity and movement of people, triggering an explosion of infections and deaths.
Figure 1: Circles are sized by the number of people there who have tested positive as of 27 April 2020.
Sources:The New York Times[19]
However, despite these efforts and boasting of some of the most advanced healthcare infrastructure in the world, New York City, as well as the rest of the US, is facing a severe shortage of medical equipment.[20]
The inability of New York City’s healthcare system to keep pace with the massive number of COVID-19 cases could well be attributed to its population density. The city’s population has grown by over one million since 1990,[21]with a population density increase of over 27,000 people per square mile (roughly 17,000 people per square kilometre).[22]As one of the most expensive cities in the world by real estate standards, most of the migrant population is forced to live cheek by jowl in New York City’s hidden slums.[23]
Uneven Growth, an urban design exhibition at the Museum of Modern Art from November 2014 to May 2015, highlighted how the affordability crisis had created a vast informal rental market where illegally subdivided existing apartments to accommodate the city’s poor was rampant.[24]The displays exhibited heatmaps of nearly 200,000 illegally subdivided hyper-dense dwellings—apartments, basements, attics, lofts and industrial sheds—across New York City, which in other metropolitan areas, such as Mumbai or Rio de Janeiro, would be identified as ‘slums.’ Concentrated mainly in the outer regions of Queens, the Bronx, and eastern Brooklyn (all COVID-19 hotspots within the city),[25]these illegal living quarters mainly provide shelter to scores of undocumented immigrants.[26]The informal nature of this particular housing market makes it difficult for tenants to claim basic housing rights that exist in other parts of the city.[27]
New York City’s high population density also translates to a high degree of public transport use for daily commutes. The delay in announcing comprehensive lockdown measures meant that the Metropolitan Transport Authority, North America’s largest multimodal transport network, continued to cater to its daily 8.6 million riders for several days after the initial outbreak, further accelerating the spread.[28]
What could be the cause for New York City emerging as the US’s COVID-19 epicentre? AWashington Postreport indicated a link between the region’s density and confirmed cases. “None of the most lightly populated counties has confirmed cases; most of the counties with the highest population densities have confirmed cases,” it said.[29]
London
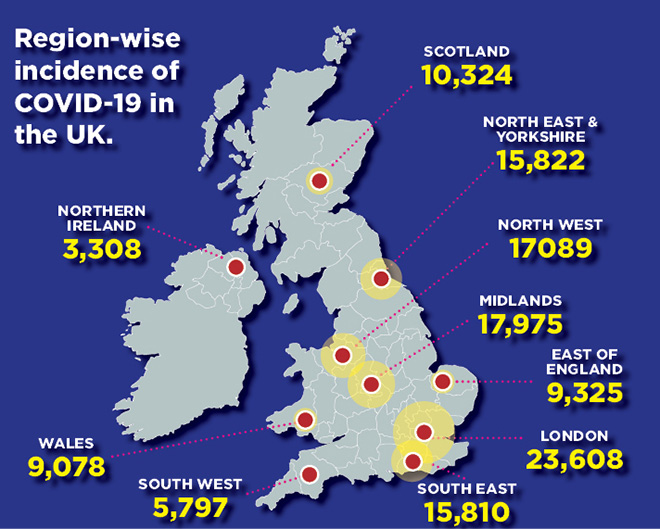
London has the most number of positive COVID-19 cases and deaths caused by the disease in the UK. As of 27 April, the UK reported over 157,000 positive cases,[30]nearly a fourth of which were in London. London has also accounted for almost one-fifth of all deaths in the UK.
Figure 2: Incidence of COVID-19 cases.
Source:The Sun[31]
As of 2019, its overall population density was less than 6,000 people per square kilometre.[32]However, the city shows huge disparities when it comes to densities within its boroughs. Data released by the Greater London Authority shows that, of Greater London’s 32 boroughs, as many as 12 in Inner London have a population density of over 10,000 people per square kilometre.[33]The boroughs of Hackney, Islington and Tower Hamlets have densities of close to 16,000 people per square kilometre, while in Kensington and Chelsea, Lambeth, Hammersmith and Fulham, Southwark and Westminster, the density is close to 13,000 people per square kilometre. Inner East and South London have the highest average population density of all of London’s sub-regions, at 11,200 people per square kilometre.[34]
Such high degree of disparities in the population densities of the different boroughs makes London an ideal case to study how the highly skewed population distribution within the diverse city areas have acted as ‘clusters’ for the spread of the virus. For instance, when the infection first establishes in a high-density area, anyone who meets the host becomes susceptible to the virus. Some of these persons may get infected, but remain asymptomatic and continue to mingle around without any precaution, eventually creating small clusters of the contagion within the dense population of the area. The infections spread as these people travel to the less dense parts of the city.
Many people from hyperdense clusters travel long distances for work to the more well-endowed areas/suburbs/boroughs daily. This mostly urban phenomenon is the primary cause of concern as cities are struck with a virus that has the potency to spread among entire populations quickly. This is true for almost all the megacities cities across the world that have experienced the current outbreak; infections have spread across cities on the whole and are not isolated to individual parts. The spread of COVID-19 has been far beyond global financial centres and megacities and has impacted the global production, supply and consumption networks that cover most of the urbanised world.[35]
London is among the world’s most expensive property markets and also has the highest rent to income ratio of any region in the UK.[36]A large number of families spend over a third of their income on rent, leading to undesirable consequences on other quality of life parameters.[37]High rents have also become a significant cause of poverty and inequality in London. In the three years leading up to 2016, London had 960,000 private renters living in poverty.[38]Over half of all children living in private rented housing are in a state of poverty.[39]
The peculiar situation in London has forced thousands of families to live in miserable slum-like conditions. Since 2011, the number of homeless in temporary accommodation grew by 25 percent, while the number of families in night shelters and bed-and-breakfast lodges have more than doubled.[40]London also faces a high-degree of homelessness, with the number of homeless people increasing by 165 percent since 2010.[41]
The National Health Service (NHS), one of the best public health systems among the Commonwealth countries,[42]has been overwhelmed by a “continuous tsunami” of COVID-19 patients.[43]The NHS is struggling to meet the “explosion of demand,”[44]despite increasing critical care capacity in London hospitals by between five and seven times in the past few weeks. Health workers have sounded “alarm bells” about the dwindling stock of personal protective equipment (PPE).[45]London also has a shortage of 30,000 ventilators and efforts to procure the required number are falling short.[46]
As in any other megacities, public transport in London is the city’s lifeline. More than three million Londoners use public transport for their daily travels.[47]For several days after the lockdown was announced, the city’s tube trains continued to operate at full frequency and capacity, mostly ferrying people for non-essential work such as construction.[48]
Urban densities and COVID-19: The Case of India
India’s urban population grew from 25,851,873 in 1901[49]to over 377,000,000 in 2011,[50]a 1,358-percent rise. But the process of urban planning and resource management has failed to match this population growth. As a result, an increasing number of people live in informal settlements across the country’s urban areas. Nearly half of Mumbai’s population, for instance, live in slums.[51]
Decadal growth of urban population in India
Census year
No. of Urban agglomerations/Towns
Urban Population
1901
1,830
25,851,873
1911
1,815
25,941,633
1921
1,944
28,086,167
1931
2,066
33,455,989
1941
2,253
44,153,297
1951
2,822
62,443,934
1961
2,334
78,936,603
1971
2,567
109,113,977
1981
3,347
159,462,547
1991
3,769
217,551,812
2001
4,378
285,354,954
2011
5,350
377,000,000-plus
Source:Census 2001 and 2011
Rapid population growth in India’s urban spaces over the decades has meant that the cities have had grapple with increasing pressure on their already stretched resources.
Sr. No.
City
Population in 1951
Population in 2011
Population growth
1
Mumbai
2,966,902
16,434,386
454%
2
Delhi
1,744,000
12,877,470
638%
3
Kolkata
2,956,475
13,205,697
347%
4
Chennai
1,416,056
6,560,242
363%
5
Bengaluru
778,977
5,701,446
632%
6
Hyderabad
1,085,722
5,742,036
429%
7
Ahmedabad
788,300
4,525,013
474%
8
Pune
488,419
3,760,636
670%
India’s largest citiesSource:Census data and ORF,[52]population density and growth calculated by the author from available Census data.
Considering that the land area of India’s eight largest cities has remained the same, the scale of population growth has resulted in unmanageable and unsustainable densities per square kilometre. In Mumbai, for instance, about 2,000 people occupied one square kilometre in 1901, increasing to 9,000 people in 1961, over 20,000 in 1991,[53]and 28,000 per square kilometre in 2011.[54]Mumbai has also seen a steady reduction in the availability of space per capita, from 500 square metres in 1901 to 111 square metres in 1961 and 36 square metres in 2011.[55]Meanwhile, Dharavi has over 200,000 people per square kilometre.[56]
Healthcare in urban India
According to the 2019 National Health Profile, India currently has 713,986 beds—or 0.55 beds per 1,000 people—in government hospitals.[57]Of these, only 5-8 percent—an estimated 35,699-57,119—are ICU beds, while those with ventilators, at an optimistic estimate of 50 percent of all ICU beds, are only about 17,850-25,556.[58]Even if the private sector infrastructure were to be included in this capacity, India would still need 80 to 100 times the available number of ventilators if one considered a “worst-case scenario”.[59]
The majority of private sector healthcare is limited to large cities. Its adequacy will be put under strain as cities are most likely to emerge as COVID-19 hotspots. Mumbai has around 800 ventilators in the state-run and municipal hospitals and an additional 800 in private hospitals.[60]States such as Tamil Nadu and Madhya Pradesh have 1,500 and 1,800 ventilators respectively in government hospitals; Kerala has 5,000.[61]Most of these ventilators are already in use for other critically-ill patients and will be unavailable in case of a significant increase in demand for COVID-19 patients.
The most significant risk to India, however, is in terms of testing. It is reasonable to conclude that New York and London have registered a large number of COVID-19 cases because they are well-equipped with adequate testing infrastructure. But the shortage of testing equipment in India may be masking the real picture.[62]The urban population densities will only amplify this shortage if the virus were to spread at the community-level. In Mumbai’s Dharavi, for instance, which has a population of 8 lakh living in a total area of 2.1 square kilometres and where 220 cases have already been identified,[63]it will be impossible to test everyone if there were community transmission. With India still in the second stage of COVID-19 transmission, isolation and contact tracing remain the backbone of the response strategy. India must urgently broaden its testing strategy, which currently targets only a subset of symptomatic people—those who travelled internationally or have come in contact with laboratory-tested positive patients.[64]Without aggressive testing, lockdowns, social distancing and frequent handwashing may only be able to contain the transmission temporarily. The incidence of the COVID-19 disease may see a sudden spike as many symptomatic, but untested, persons turn positive. In such a scenario, high densities will only aggravate and intensify the spread of the infection, without preventive measures
India’s first COVID-19 case—a patient who had returned from Wuhan, China, where the virus originated—was confirmed at the end of January.[65]The country’s first coronavirus-related death—a person with a history of travel to Saudi Arabia—was reported on 11 March.[66] The disease has continued to spread across India. As of 28 April, India had 29,435 confirmed COVID-19 cases and 934 deaths. The US, on the other hand, has seen about 2,000 new confirmed cases daily.[67]
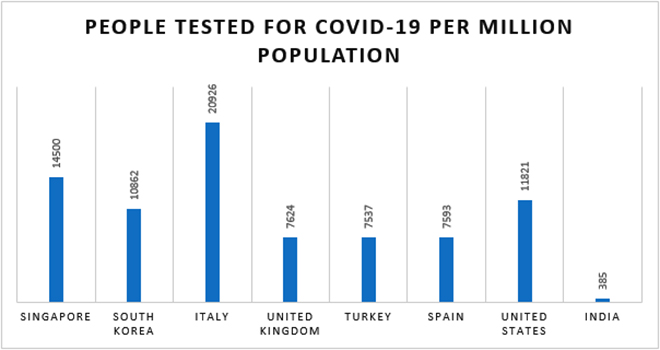
The slow testing rate in India could be the reason for the steady but slow spread of the virus in the country. The US has tested nearly a million people but has still been criticised for “being behind on coronavirus testing”.[68]The much smaller South Korea has tested close to 400,000 people.[69]Reports suggest that Norway, with 14,537 tests per million people, tops COVID-19 testing rates, followed by South Korea (7,353) and the US (1,647). Meanwhile, India, as of 24 April, had conducted 500,000 tests, at 385 tests per million people.[70]This is a promising increase from the negligible tests count of just 18 per million people on 26 March.
Note:Data from Singapore based on testing numbers from 20 April, for India from 25 April and for other countries from 18-20 March. Source:Scroll.in,[71]Businessinsider.com,[72]ORF Coronavirus Tracker, Our World in Data, ICMR, media reports
A study published before the countrywide lockdown by researchers at the Indian Council of Medical Research (ICMR) and the Department of Infectious Disease Epidemiology at Imperial College, London, warned that community transmission of COVID-19 may take anywhere from 20 days to a few months to be visible and that every infected Indian will pass the virus to 1.5 persons in the best-case scenario and four persons in the worst-case scenario.[73]The study was based on mathematical modelling of the number of airport screenings of incoming travellers from abroad. It predicted that controlling the spread of the virus would be difficult in “pessimist” scenarios in Delhi, Mumbai, Kolkata, Bengaluru, Chennai, Hyderabad and Kochi—all high-density cities.
Efforts are being made to ramp up both testing facilities and critical hospital infrastructure in a bid to avoid the worst-case scenario. The Modi government has also sanctioned INR 150 billion to strengthen India’s public health infrastructure.
According to a health ministry communique, as of 6 April, India has received 170,000 PPE kits from China, which along with 20,000 PPE coveralls procured domestically, have been distributed to hospitals across the country, especially to those states with a high incidence of COVID-19 cases. Of the 387,473 PPEs available in the country, the Indian government has arranged for and supplied a total of 294,000 PPEs.[74]Since 30 March, India has added nearly 34,500 PPE kits to its national inventory.[75]Phased supplies from the orders for 8 million PPE kits (including N95 masks) from Singapore are also expected to begin soon, while the government is at an advanced stage of negotiations with a Chinese firm for an order of 60 lakh complete PPE kits, which will also include N95 masks.
The ICMR has boosted this capacity by approving the procurement of one million testing kits and also 700,000 RNA extraction kits,[76]from a slew of local manufacturers.[77]India’s critical care infrastructure, too, is being strengthened, with auto giants Mahindra & Mahindra and Maruti planning to manufacture cost-effective ventilators at some of their production facilities.[78]Bharat Electronics Limited, a public-sector undertaking, is also collaborating with other local manufacturers in this endeavour.[79]
But even if the government manages to overcome the shortfall of basic PPE kits and critical care medical equipment, it has another challenge to tackle—the number of doctors and nurses. According to the World Health Organization (WHO), India has a low doctor to patient ratio, with only 8.57 doctors per 10,000 people.[80]
Country
Year
Medical doctors (including general practitioners, specialists & others)
Medical doctors/ 10,000 people
No. of positive cases up to 24 April 2020
United States
2017
1,698,252
26.12
902,582
Italy
2018
482,272
39.77
192,994
Spain
2017
361,326
38.72
219,764
Germany
2017
702,390
42.48
150,383
China
2017
2,828,999
19.80
82,816
France
2018
424,674
32.67
114,657
Iran
2018
259,208
15.84
89,328
United Kingdom
2018
377,078
28.11
148,377
Switzerland
2017
72,648
42.95
28,894
Turkey
2017
299,994
18.49
107,773
India
2018
1,159,309
8.57
24,942
Source:Compiled by the author based on data from Global Health Observatory Data Repository, WHO, April 2020
Can urban densities be controlled? Lessons from China
There is much to learn from China and its containment of the COVID-19 virus, despite its mistakes in the early stages of the pandemic.[81]Some of the aggressive steps taken by the Communist Party of China to control migration and tackle city densities may not be feasible for liberal democracies such as India and the US to emulate, but urban population densities cannot be left to grow uncontrolled.
Well-planned cities can have immense benefits because of the scale that densities provide, but they also become vulnerable, exclusive, unsafe and defenceless to tackle natural or humanmade disasters of the size and magnitude of the COVID-19 pandemic. So, while copying China’s policies is ill-advised, it is worth studying them for some insight on how to strengthen megacities.
The hukou (household registration) system
China owes much of its impressive, though mostly uneven, economic growth and technological achievements over the past 20 years to thehukousystem, a household registration programme that regulates population distribution and migration to urban areas.
Today, China has about 1.4 billion people living in 34 administrative regions at the provincial level—23 provinces, four municipalities, five autonomous regions, and the two special administrative regions of Hong Kong and Macao.[82]These 34 administrative units have a total of 675 cities, with about 350 million urban residents or non-agricultural hukou holders, or 26.1 percent of the total population. These administrative regions are further divided in multiple ways to enhance their management and control population growth.
In all of China’s administrative areas, thehukoustatus determines where a person can live and work, how much they earn, where their children attend schools, and whether they can avail state subsidies for education and medical care, among other things. While thehukouis centrally-governed, its implementation is almost entirely managed by the provincial governments and municipalities through regulations, directives and decrees as per the region-specific requirements—all under the ambit of the Central agenda.
There are four principles governinghukourelocation and internal migration in China:[83]
To strictly control any migration that changes agricultural or ruralhukouto non-agricultural or urbanhukou, townhukouto cityhukou, or cityhukouto metropolitanhukou(Beijing, Shanghai and other major cities).
To control migration appropriately from the countryside to suburban areas, from suburban areas to cities, or from small cities to large cities.
To allow parallel migrations between or exchanges ofhukouzones in similar villages, comparable towns, or similarly ranked cities.
To encourage dispersal from cities to towns, from large cities to small cities, and from urban areas to the countryside.
While some of these objectives might appear similar to the provisions for zoning and land-use reservations made in city development plans, where thehukousystem differs is the way it unfairly segregates the population on the urban-rural and economic lines. Thehukouis nothing but an organised way to divide and exclude people and ensure that internal migration and the urban population are kept under check.[84]
However, major reforms aimed at softening thehukousystem’s vice-like grip are being made under the leadership of Chinese President Xi Jinping.[85]In a policy statement issued in December 2019, the State Council pledged to eliminate the registration system in all cities with fewer than three million residents and relax it in cities with populations of up to five million. The statement also said that for megacities, such as Beijing and Shanghai, the household registration system would be simplified.[86]
The relaxation of hukou will help China speed up its urbanisation process and allow more people from the countryside to live and work in the cities without compromising their human dignity. The reforms are sought to provide a “new engine for the slowing economy” as increased urbanisation will move people to its Tier 2 and 3 cities where opportunities exist to contribute to the nation’s economic growth.[87]
While doing away with restrictions on migration to smaller cities, severehukourestrictions will continue in the Tier 1 megacities such as Beijing, Shanghai, Guangzhou and Tianjin. For these cities, China has put in place an additional strategy to reduce population densities.
Population bariatrics in Beijing and Shanghai
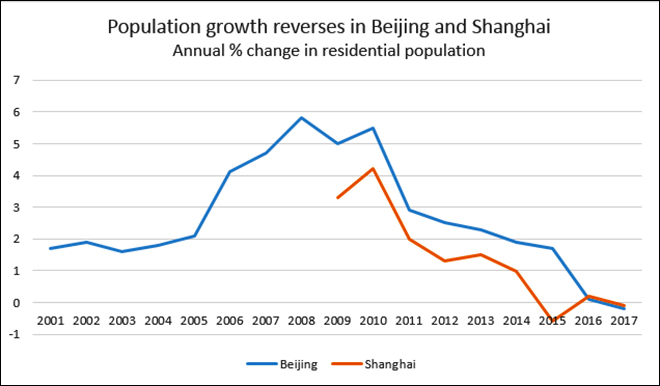
In 2016-17, China embarked on a mission to cut the population flab in Beijing and Shanghai and address the‘Chéngshì Bìng,’or ‘big city disease’. Around mid-November 2017, the municipal governments in both megacities began mass demolitions of ‘illegal housing’ after a fire in a crowded Beijing district. All illegal structures, mostly shops and homes of low-income residents spread over an area of 15 square miles, were razed[88]in a bid to force migrant workers with ‘outside’ non-urbanhukou—blamed for overcrowding and the rising crime rate—out of the city, although the official media maintained that the primary goal was to eliminate safety risks.[89]The local administration was simply implementing a decision to cap the population of Beijing at 23 million by 2020[90]and that of Shanghai at 25 million by 2035,[91]an idea formulated after data from the National Bureau of Statistics showed that resident population in Beijing had skyrocketed by 59 percent and in Shanghai by 50 percent in the past decade.[92]
The demolition drive accelerated the ‘redistribution’ of migrants, sending them packing far beyond the Beijing and Shanghai city limits. While the human cost of such swift and decisive action must be denounced, it should also be considered that China is convinced that some bold measures to control urban populations are essential to ensure the long-term survival of cities.
Besides the forced redistribution, the plan to limit city population growth involves the diffusion of people into new urban areas, such as the Jing-Jin-Ji region outside Beijing, and the 39-square mile Xiong’an New Area, a new city district near Hebei, being developed as new tech hubs.[93]
The slow gains reaped through the soft methods of dispersing excessive city population to the outskirts by spreading economic activity got a powerful thrust with the adoption of the hard ‘redistribution’ steps, practised through the mass demolitions. As per Beijing’s 2018 Population Development and Study Report, the population of Beijing decreased by 22,000 year-on-year to 21.7 million, a decline of 0.1 per cent.[94]Shanghai’s population dropped marginally for the first time in 20 years, by 13,700 to 24.18 million.[95]
Source:Financial Times[96]
Optimal population density
Liberal democracies cannot emulate China’s methods in dealing with city densities. But policymakers should not ignore the lessons that can be learnt by studying the Chinese policies to boost the overall sustainability, safety and liveability of cities. Large populations provide cities with the critical mass to ensure socio-economic development and enhance productivity. They provide the scale that ensures the per-unit cost of the greedy capital-intensive infrastructure development remains economical. They utilise resources and increase the viability and efficiency of services, including public transport, energy use and housing. But population densities also create higher levels of pollution, provide fertile ground for the uncontrolled proliferation of slums, and greater congestion and expensive real estate. Increasingly denser cities thus become exclusive, inequitable, unhealthy and environmentally unsustainable.
When densities breach their critical mass, they have negative consequences on economic, environmental and social sustainability. Do cities provide their people with equal economic opportunities? Do people lead healthy lives in terms of safe water, air, transport, education, health, markets, open spaces, and recreation? Do cities deliver equal employment opportunities so that all people, rich and poor, find meaningful working and living space in the city? Cities must urgently quantify an optimal population density—the critical mass—which, if breached, would directly impact their economic, environmental and social sustainability. For their survival, India and other countries dealing with enormous densities must factor in population in “pre-determined planning strategies, not in post-development excision.”[97]
Recommendations
The United Nations’2016 World Cities Reportrecommended that the pattern of urbanisation across the world needs to change to better respond to contemporary challenges address issues such as inequality, climate change, informality, insecurity, and the unsustainable forms of urban expansion.[98]While the report proposed what it called a ‘New Urban Agenda’ to make cities sustainable in terms of equity, economy and environment, it failed to identify the perils that high population densities—especially in packed urban sprawls—can pose in times of large-scale humanitarian crisis. As a result, it fell short of making adequate recommendations for containing the explosion in urban populations.
The following recommendations can help countries be better prepared to address the uncontrolled densities in their urban agglomerations.
Cities must abandon the practice of planning based on population projections that are derived from current demographic patterns. Populations that are bound to rise for several decades beyond the plan period make such planning flawed and redundant by the time its term ends. The imperative is a thorough re-evaluation of all existing city development plans from a lens of an ‘optimum population projection’ that suits the Indian context. Most public amenities and infrastructure—especially housing, roads and open spaces—and most utilities—water and sanitation, sewage treatment and disposal—become ineffective and disorderly when the population outgrows their projected use. For such infrastructure and amenities, optimum land needs to be provided from the beginning for an optimum population.
Decentralised urbanisation holds the key to healthy urban growth. Decentralised governance will assist several viable cities to grow and share amongst them the urbanisation pressures that are currently concentrated on a handful of urban centres. One way to do this is to streamline the Integrated Development of Small & Medium Towns scheme from the point of view of densities with greater financial capacity, functional liberty, and empowerment.
The different standards adopted by different states and cities must be studied to arrive at optimum densities to institute realistic national standards for city amenities. The government must redefine its Urban and Regional Development Plans Formulation and Implementation guidelines to account for possible space distribution for various uses in the socio-economic context of an urbanising India.
India, as one of the world’s fastest-growing economies, has not been able to translate the gains of urbanisation into rural development, in general, and agricultural development, in particular. The fact that 59 percent of the country’s total workforce is employed in the agricultural sector, which accounts for just 23 percent of GDP,[99]reflects the erosion of the mechanisms by which growth witnessed by India’s urban centres percolates into rural areas. Priority must be accorded to the implementation of schemes such as the Shyama Prasad Mukherjee Rurban Mission (SPMRM), which aim to develop growth clusters in rural areas by providing social, economic and physical infrastructure. With its objective of harnessing the potential of growth in these rural clusters by capitalising on the economic drivers of urbanisation, and leveraging locational and competitive advantages, the SPMRM can provide stimulus to arrest the uncontrolled rural-to-urban migration. Likewise, other programmes that can optimally harness balanced and inclusive urban growth and development to create better opportunities in rural India must be explored to help those rural areas urbanise.
The vast variance in the densities of London’s boroughs mirrors the unequal distribution of population densities in almost all global megacities. Though the traditional planning strategy of segregation eventually gave way to a mixed-used development, no effort has been made to devise a strategy to address the issue of population density. In developing countries, owing to the saturation of cities, the urban sprawl is much more than just land being appropriated by slums. It is now a practice of urban agglomerations that usurp large parts of neighbouring peri-urban and rural areas for their expansion. Where and how this new land is incorporated into the urban matrix will determine the social and environmental well-being of future populations. The developing nations, which are slated to drive global urbanisation in the coming decades, need to pay due attention to this aspect.
As India and other developing countries continue to urbanise, increasing numbers of the rural poor will migrate to the megacities in search of informal employment. It is time these cities revisit their urban strategies and revise their urbanisation processes and practices. The overhauled urban strategies must look beyond the myopic gains of the political economy, view the slum populations beyond their role as mere ‘vote banks,’ work against hyper densification through spatial policy interventions, and discard archaic land-use policies and rent laws. Most importantly, the New Urban Agenda needs to be tailored to the needs of the urban poor to allow them equal access to basic amenities and services. In framing such a new urban policy, countries must introspect on how, over the years, the urban poor have been pushed farther to the margins in their crowded and unhygienic ghettos. The millions who live in the urban sprawls clustered across the city landscape end up being overlooked in the provision of services—clean and assured water supply, sanitation, healthcare, education and other basic quality of life indicators—as city planners pursue their aims of building ‘sustainable’ cities. Such hidden tendencies reflect poorly on the ‘liberal’ ethos of democracies, making them no different from the apparent ‘draconian’ policies of socio-economic exclusion and division practised by authoritarian regimes.
Conclusion
The industrial revolution of the 19thcentury spurred the growth of slums, inspiring planners to imagine lower-density settlements. The garden cities of the UK paved the way for urban settlements with tight control on densities, giving benefits of access to open space. The 20th-century modernist architects also placed population density control at the core of their designs. The efforts to keep urban densities under control were also evident in the post-war rebuilding programme, where the notion of towers in the park held a strict limit on dwellings per hectare. It was only in the age of modernist urbanism that the aversion to densities was overturned, eventually leading to a global explosion of high-density urbanisation.
Diseases have also had a defining role in urban development trends over the centuries. Whether the mid-19thcentury cholera outbreaks that led to the establishment of London’s Metropolitan Board of Works and modern sanitation systems, or the 1896 Bombay plague that led the Britishers to reclaim land to stitch together the seven islands that make present-day Mumbai, epidemics have charted the growth of cities across the world.
The harsh interventions implemented in India may be successful in mitigating the spread and local transmission of COVID-19. However, much more determined work is required to achieve an optimum balance between the expected positive effect on lives saved and the negative impact on freedom of movement, the economy and society at large. Over the short- to medium-term, India and other countries must find the political will to address the increasingly unmanageable population densities of their urban agglomerations. The task is not easy, but COVID-19 may not be the last of the pandemics that the world will see. It will be unwise to not allow nature to restore its balance.
Endnotes
[1]Ed Glaeser, “The Benefits of Density”,Urban Age, 2012.
[2]David Simon, “Cities are at centre of coronavirus pandemic – understanding this can help build a sustainable, equal future”,The Conversation,23 April 2020.
[3]Nace, Trevor, “Population Adjusted Coronavirus Cases: Top 10 Countries Compared”, Forbes, 2020.
[4]UN Department of Economic and Social Affairs (2018). “2018 Revision of World Urbanization Prospects”.
[5]UN HABITAT (2012), “State of The World Cities 2012/2013 Prosperity of the Cities”.
[6]UN Department of Economic and Social Affairs, (2018). “2018 Revision of World Urbanization Prospects”.
[7]UN HABITAT (2012). “State of The World Cities 2012/2013 Prosperity Of The Cities”.
[8]Joel Kotkin, “After coronavirus, we need to rethink densely populated cities”,Fortune, April 2020.
[9]“Coronavirus: Significant social distancing needed ‘until vaccine found”,BBC News, 16 April 2020.
[10]Rashid, Omar, “Coronavirus: Despite U.P. CM’S Appeal, Migrant Workers Throng Lucknow’s Bus Stands”, The Hindu, 2020.
[11]Rupam Jain, “India rolls out coronavirus call centers to stop stampede to hard-pressed hospitals”, Reuters, March 2020.
[12]Annika Blau and Simon Elvery, “Coronavirus: How deadly and contagious is this COVID-19 pandemic?”,ABC News, 2020.
[13]Arcadis,Design and Consultancy for natural and built assets, Sustainable Cities Index, 2016.
[14]“Coronavirus in The U.S.: Latest Map and Case Count”, The New York Times, 2020.
[15]Maslin Nir, Sarah, “Coronavirus in N.Y.: Inside New Rochelle’s ‘Containment Area’”, The New York Times, 2020.
[16]Rowland, Christopher, & Ariana Eunjung Cha, “Surge in Corona Virus Patients Threatens to Swamp U.S. Hospitals”, The Washington Post, 2020.
[17]Martinez, Luis, “Army Helps Make Temporary Hospital At New York’s Javits Center One of the Largest in the Country”, ABC News, 2020.
[18]Andy Sullivan, “Trump drops idea of New York lockdown as U.S. death count crosses 2,000”,Reuters, March 2020,
[19]“Coronavirus in the U.S.: Latest map and case count”,The New York Times, April 2020.
[20]Chapman, Ben, and Jimmy Vielkind, “New York City Faces Challenges as U.S. Epicentre for Coronavirus”, Wall Street Journal, 2020.
[21]NYC Department of City Planning (2020). “New York City Population”.
[22]Ibid.
[23]Ferro, Shaunacy, “A Heat Map Of New York City’s Hidden Slums”, Fast Company, 2014.
[24]World Architecture Community (2014). “Uneven Growth: Tactical Urbanisms For Expanding Megacities”. 2014.
[25]Austin Horn, “U.S. Coronavirus Death Toll Passes 50,000”,NPR, 24 April 2020.
[26]Ferro, Shaunacy, “A Heat Map Of New York City’s Hidden Slums”, Fast Company, 2014.
[27]Ibid.
[28]Metropolitan Transport Authority (2018). “The MTA Network: Public Transportation For The New York Region”.
[29]Bump, Philip, “New York City Is the Epicentre Of Coronavirus in The U.S. – Is This Due to Density Or Testing?”,The Washington Post, 2020.
[30]“Coronavirus UK map: How many confirmed cases are there in your area?”,BBC News, 27 April 2020,
[31]Official UK Cases & Deaths – Accurate as of April 27,The Sun, 27 April 2020,
[32]Trust for London (2017). London’s geography and population.
[33]Greater London Authority (2018).Land Area and Population Density, Ward and Borough.
[34]Trust for London (2017). London’s geography and population.
[35]Ibid.
[36]Mayor of London, Office of National Statistics (2020). “Index of private housing rental prices, Region”.
[37]Ella Willis, “Londoners spend more than a third of monthly income on rent, study finds”,Evening Standard, 2018,
[38]Ibid.
[39]Trust for London (2017).Child poverty and housing tenure.
[40]Office of National Statistics (2019).UK homelessness – 2005 to 2018.
[41]Wainwright Daniel, “Homelessness: Rough sleeping five times higher than official figure”, BBC News, 2020.
[42]Denis Campbell, “NHS holds onto top spot in healthcare survey”, The Guardian, 2017.
[43]“Coronavirus: Rishi Saunak to unveil financial aid for self-employed”,BBC News, March 2020.
[44]Ibid
[45]John Tara, “‘Like a bomb had gone off on either side of their chest’ London doctors speak of ‘continuous Tsunami’”,CNN, March 2020.
[46]Thomas Colson, “UK hospitals will be given just 30 of the 30,000 extra coronavirus ventilators they urgently need next week”, Business Insider, April 2020.
[47]Clough Freestone Richard, “The millions of people who use public transport in London every day deserves a frequent, comprehensive, and fairly priced service”, London School of Economics, February 2012.
[48]Mason Rowena, Murphy Simon, Morris Steven, Parveen Nazia and Lisa O’ Carroll, “No. 10 criticised after unclear lockdown advice confuses public”, The Guardian, March 2020.
[49]Office of the Registrar General, India (2001). “Variation in urban population since 1901”.
[50]Office of the Registrar General, India, 2011, “Census of India 2011”.
[51]Bendix, Aria, “Drone Photos of Mumbai Reveal The Places where Extreme Poverty Meets Extreme Wealth”, Business Insider, 2019.
[52]Ramanath Jha, “Decentralised urbanisation holds key to healthy urban growth”, ORF, May 2018.
[53]Ibid., Census of India 2001, 2011.
[54]Urban Hub (2015).
[55]Ramanath Jha, “Decentralised urbanisation holds key to healthy urban growth”, ORF, May 2018.
[56]Murphy, Douglas, “Where is the World’s Densest City?”,The Guardian, 2017.
[57]Central Bureau of Health Intelligence, Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India (2019). “National Health Profile 2019, 14th Issue”.
[58]Singh Prachi, Ravi Shamika, Chakroborty Sikim, “COVID- 19| India’s health infrastructure equipped to handle an epidemic?”, Brookings, March 2020.
[59]Chandna Himani, “India has 40,000 ventilators but could need many more in ‘worst-case scenario’”, The Print, March 2020.
[60]Marpakwar Chaitanya, Mishra Lata, “Govt foresees shortfall, Orders 150 ventilators for corona patients.”Mumbai Mirror, March 2020.
[61]Chandna Himani, “India has 40,000 ventilators but could need many more in ‘worst-case scenario’”, The Print, March 2020.
[62]“India’s poor testing rate may have masked coronavirus cases,”Al Jazeera, March 2020.
[63]Saurabh Gupta, “Coronavirus: Mumbai’s Dharavi, A COVID-19 Hotspot, Reports Sharp Drop In New Cases”,ndtv.com, 25 April 2020.
[64]Oomen Kurian, “To test or not to test: How is India navigating the double bind?”, ORF, March 2020.
[65]Reid David, “India confirms its first coronavirus case”, CNBC, January 2020.
[66]“India’s first coronavirus death is confirmed in Karnataka”,Hindustan Times, March 2020.
[67]Joel Shannon, “Coronavirus is spreading so quickly that our brains can’t keep up. Experts explain why”, USA Today, March 2020.
[68]Thomke Stefan, “Why is the U.S. Behind on Coronavirus Testing?” Harvard Business Review, March 2020.
[69]Prabhash K Dutta, “Is coronavirus situation in India less severe than other countries?”,India Today, March 2020,
[70]Ruchika Chitravanshi, “Govt says rise in Covid-19 cases linear, not exponential; wants more tests”,Business Standard, 24 March 2020.
[71]Arunabh Saikia, “Testing is key to fighting coronavirus, so why does India have such a low testing rate?”,Scroll.in, March 2020.
[72]Aylin Woodward, Shayanne Gal, “One chart shows how many coronavirus tests per capita have been completed in 6 countries. The US has finally caught up”. Businessinsider.in, 21 April 2020,
[73]Mandal S, Bhatnagar T, Arinaminpathy N, Agarwal. A., Chowdhury A, Murhekar M, March 2020, “Prudent public health intervention strategies to control the coronavirus disease 2019 transmission in India: A mathematical model-based approach”, NCBI.
[74]Ministry of Health and Family Welfare (2020). “Updates on COVID-19 – Outsourced supplies of PPEs begin landing in India”.
[75]Ministry of Health and Family Welfare (2020). “COVID19 Update: Availability of PPE kits, N95 masks and ventilators”.
[76]Joe C Mathew, “India readies massive COVID-19 testing plan”, Business Today, March 2020,
[77]Anu Ranganathan, “India Ramps Up Coronavirus Testing, Approves Slew Of Local Test Kit Makers”,Forbes, 16 April 2020.
[78]Banerji Sumant, “Coronavirus: Here’s how Mahindra, Maruti will produce ventilators at plant”, Business Today, March 2020.
[79]Ministry of Health and Family Welfare (2020). “COVID19 Update: Availability of PPE kits, N95 masks and ventilators”.
[80]WHO, March 2020.Global Health Observatory Data Repository.
[81]Jeremy Page, Wenxin Fan, Natasha Khan, “How It All Started: China’s Early Coronavirus Missetps”, The Wall Street Journal, April 2020.
[82]China Legal Information Centre (2017).“What is the administrative division system of China?”.
[83]Fei-ling Wang, “Organising through division and exclusion – China’s hukou system,” 2005, Stanford University Press
[84]ibid
[85]“China Loosens urban residency restrictions to spur Growth”,Bloomberg Quint, January 2020.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Dhaval is Senior Fellow and Vice President at Observer Research Foundation, Mumbai. His spectrum of work covers diverse topics ranging from urban renewal to international ...

 PDF Download
PDF Download