-
CENTRES
Progammes & Centres
Location
 PDF Download
PDF Download 
Sreeparna Banerjee, “The Rohingya Crisis: A Health Situation Analysis of Refugee Camps in Bangladesh”, ORF Special Report No. 91, July 2019, Observer Research Foundation.
Introduction
The Rohingyas are a minority Muslim community who have lived in the Rakhine State of Myanmar for centuries. In recent years, they have become a brutally oppressed, “stateless” community as the state of Myanmar continues to deny them citizenship under the country’s nationality law of 1982.That law, alongside other discriminatory policies set by the old junta—which ruled Myanmar from 1962 to the holding of general elections in 2010—have curtailed the Rohingyas’ basic rights, such as education, health and employment. Moreover, the state and central governments of Myanmar continuously provoke apathy and violence against the “illegal Bengalis.”Large-scale displacement and killings have been reported since the 1970s, which intensified after the communal violence of 2012 after a group of Rohingyas were charged with raping and killing a Buddhist woman. The Rohingyas were evicted from their homes, their land confiscated, and their villages and houses attacked by Myanmar’s military.In August 2017, a massive crackdown in Myanmar killed thousands of Rohingyas and triggered the mass exodus of around three-quarters of a million of them to Bangladesh.
While the Rohingyas legally fall under the category of “de jure stateless,” the Government of Bangladesh (GoB) recognises them as “Forcibly Displaced Myanmar Nationals.”Unlike other South Asian countries, Bangladesh is not a signatory to the 1951 Convention Relating to the Status of Refugees (or its 1967 Protocol), the 1954 Convention Relating to the Status of Stateless Persons (the 1954 Convention) or the 1961 Convention on the Reduction of Statelessness (the 1961 Convention).Thus, the GoB is not required to use the term “refugee” in its official documents, and the country’s judiciary system makes no provisions for refugees or stateless persons. However, there are a number of national laws as well as Constitutional provisions that cover all individuals residing in Bangladesh territory. Additionally, the 1946 Foreigners Act mentions the presence of refugees, which supersedes all other legal provisions by granting the GoB the power and discretion to decide on the scope of the Act’s application.Against this legal landscape, protection is supposedly extended to refugees through administrative mechanisms.
Bangladesh has had a long history of hosting displaced Rohingyas. In 1978, more than 200,000 Rohingyas first entered Bangladesh. While some of them stayed back, the majority returned to Myanmar due to pressure from the United Nations (UN) on the Myanmar government to take them back. During 1991–92, another influx of over 250,000 Rohingyas sought refuge in Bangladesh and were settled in the two officially registered camps at Nayapara and Kutupalong in the Cox’s Bazar district. Some of these settlers were repatriated, but many others stayed. Since then, Rohingyas have reached Bangladesh in droves. After the 2016 sectarian violence between the Arakan Rohingya Salvation Army (ARSA) and the military in Rakhine, another 70,000 Rohingyas fled to Bangladesh. The GoB allowed them to cross the borders. These refugees did not wait for government authorisation and further expanded the makeshift settlements, without proper infrastructure or services. This put a lot of pressure on the already dire situation of the camp areas. Thus, the recent addition of more than 712,179 “Forcibly Displaced Myanmar Nationals” has only exacerbated the appalling living conditions in the border areas of Cox’s Bazar.
Rohingya camps: An overview
Map 1: Refugee Sites by Population and Location Type
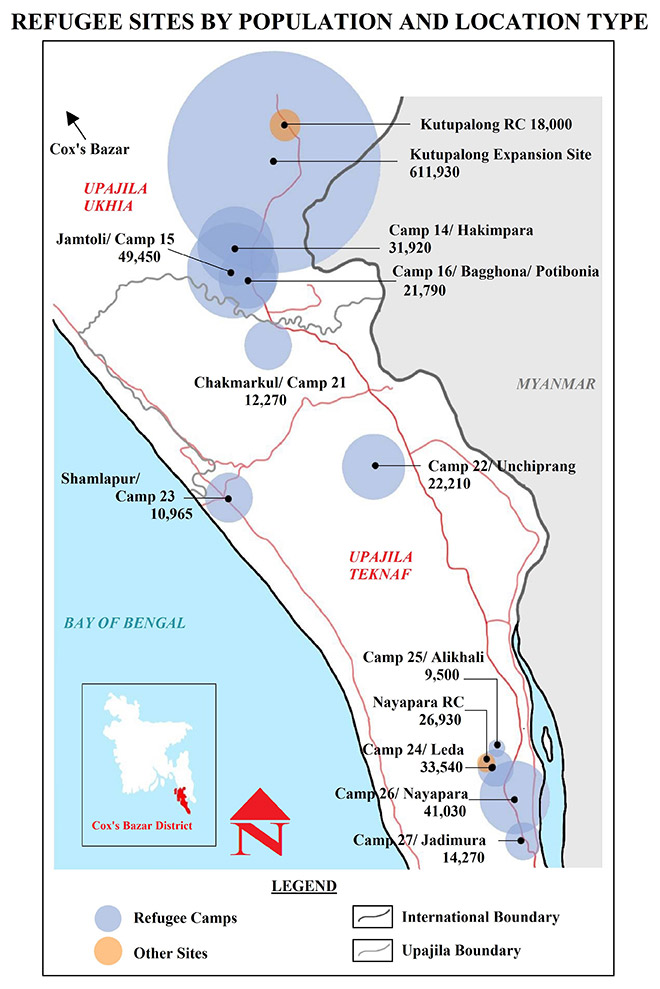
Cox’s Bazar is one of Bangladesh’s most vulnerable districts, with a poverty rate far exceeding the country’s national average.The district is prone to floods and earthquakes and is affected by approximately 40 percent of the world’s total storm surges. These natural calamities regularly undermine the local population’s safety and livelihoods.
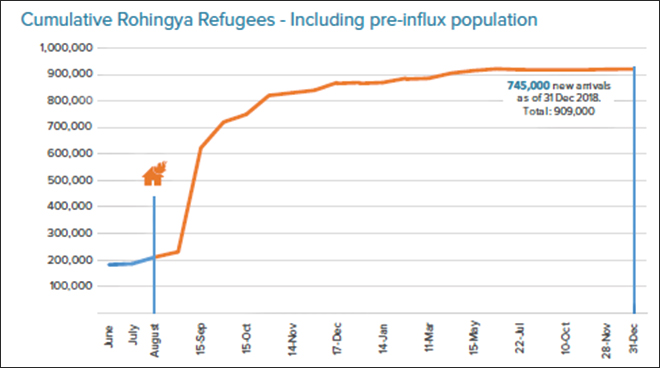
Most displaced Rohingyas are settled in the Ukhia and Teknaf areas of Cox’s Bazar, where 6,000 acres of hills and forests have been cut down to provide temporary shelters. At present, there are 34 camps housing 900,000 displaced Rohingyas, including the two officially recognised camps, Kutupalong and Nayapara. Of the other camps, some are supported by organisations such as the UN High Commission on Refugees (UNHCR) and the International Organisation for Migration (IOM).After the 2017 crisis in Myanmar, the GoB allocated a few more hectares of land close to the Kutupalong Camp to accommodate the newly displaced Rohingyas.The expansion site, along with the original camp, is called the Kutupalong–Balukhali “mega-camp”: It is the world’s largest refugee camp and hosts more than 628,500 people. The resulting population density (See Figure 1), coupled with the absence of basic services, has put immense pressure on the environment, particularly due to deforestation and depleting water resources.
Figure 1: Cumulative Numbers of Rohingya Refugees, including Pre-Influx
Historically, Bangladesh’s response to the influx of Rohingya refugees has been that of enabling humanitarian relief, assistance and repatriation. In April 2018, a Memorandum of Understanding (MoU) was signed between the GoB and the UNHCR to establish a framework of cooperation for the “safe, voluntary, and dignified returns of refugees in line with international standards.” The majority of protection-related assistance, including registration and needs assessments, has been provided by multilateral organisations, such as the UNHCR and IOM, as well as international aid organisations.
Currently, Nayapara and Kutupalong are home to some 61,700 registered Rohingyas, significantly fewer than the estimated 80,000 ‘illegal immigrants’ settled in nearby camps and local areas. The GoB, the UNHCR, non-governmental organisations (NGOs) and international NGOs provide registered settlers with cash as well as assistance in the form of shelter; education; food and cooking items such as compressed rice husk for cooking fuel, lentils and oil; and daily essentials such as soap, clothing, blankets, sleeping mats, jerry cans, WASH kits and dignity kits for women. However, unregistered Rohingyas have limited access to essential provisions and aid. Even the work opportunities created by the UNHCR and other partners in and around the two official camps are restricted to the registered settlers. Unregistered Rohingyas do not have any legal safeguards and are often arbitrarily detained. Consequently, the unregistered camps are at higher risk of violence, physical and sexual abuse, arrest and detention.
Wash concerns in the camps
Access to water, sanitation and hygiene—known collectively as WASH—includes the provision of safe water for drinking, washing and domestic activities; the safe removal of waste (toilets and waste disposal); and the promotion of healthy behavioural practices.
The Rohingyas who have been denied refugee status in Bangladesh lack access to WASH facilities. The unregistered camps are overcrowded, with few supplies and major management issues. For instance, the condition of Tal makeshift camp became so appalling that in 2008, the GoB agreed to move the Rohingyas to a better location.
While unregistered settlers are worse off, for both registered and unregistered camps dwellers, access to clean drinking water, sanitation and hygiene remains a critical concern.
1. Polluted Water
A significant WASH indicator is the reliability of tube-wells to supply an adequate quantity of safe drinking water. Reports indicate that the shallow tube-wells in the Rohingya camps supply unclean water, which the refugees have no choice but to use for drinking and other uses. Figure 2 shows that much of the drinking water in the camps is contaminated, with the quality deteriorating during the monsoon season.
Figure 2: Camp-Wise Contamination of Household Water
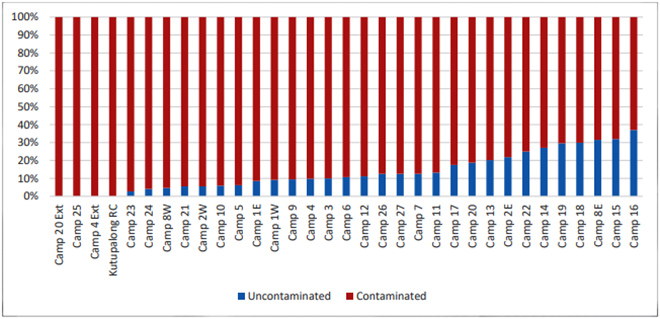
Moreover, the number of tube-wells currently available are unable to meet the increasing demands. In many camps, relief foundations supply private water tankers with taps. However, these tanks are often positioned at a highly inaccessible distance. The long queues and odd hours of availability also create security hazards for women, exposing them to harassment. Many of the settlers resort to consuming water from contaminated water bodies, such as rivers and ponds, leading to water-borne diseases in the camp areas.
As pressure increases on the aquifers in the Ukhia area, safe surface water solutions will be required to sustain the population.
2. Lack of Sanitation and Hygiene
Land shortage in the camp areas hampers effective sludge management. The latrines have shallow pits and are located close to water points, resulting in further contamination of the tube-wells. As of January 2018, more than 30 percent of latrines were located less than 10 m away from water sources. Seventeen percent of emergency latrines were either full or not functioning. Moreover, the latrines frequently remain unkempt after being used due to a shortage of water.
Many of the toilet facilities are without doors or bolts, and in some places, security lights do not function. The consequent safety risk leads community members, especially women and children, to resort to open defecation which, in turn, causes its own health and safety hazards. To avoid open bathing and defecation, some women create makeshift bathing spaces and toilets using pieces of tarp, increasing the risk of infections. They also jeopardise their health by reducing their—and their children’s—food intake to avoid frequent defecation, especially at night.
Several reports mention the unavailability of water and soap in/outside latrines, preventing proper handwash. Since soaps are expensive, personal purchase is also unlikely. Handwash is thus a gap area and needs immediate and urgent prioritisation in hygiene control.
There are no primary collection centres for solid wastes. Waste is dumped in narrow spaces between shelters and sometimes makes its way to streams. These streams are used as drinking water sources, leading to major health risks. During the monsoon season, heavy rains, landslides and flooding further disrupts WASH arrangements and endangers the overall health and well-being of the refugees.
Wash-related health risks
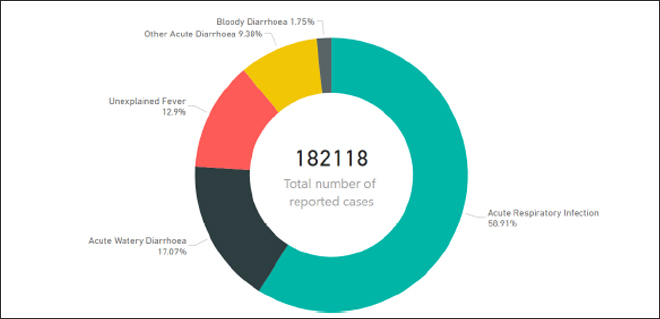
Inadequacies in WASH are responsible for a huge number of health problems amongst the Rohingyas living in camps, including diarrhoea, hepatitis, cholera and typhoid.Cholera and diarrhoea are endemic in Bangladesh and can prove fatal amongst the Rohingya populations, given their high malnutrition rates. Diarrhoeal diseases are the second biggest cause of death amongst children under five.In 2018, approximately 224,145 cases of acute watery diarrhoea (AWD) were reported.Other frequently occurring fatal diseases include acute respiratory infection (ARI), unexplained fever, bloody diarrhoea, cholera, dehydration, E-Coli and chicken pox (See Figure 3).
Figure 3: WASH-Related Cases Reported Between 4 March and 12 May 2019
In the settlements, malnutrition adds to the existing health risk due to diseases. To begin with, the refugees have come from already impoverished communities in Myanmar; their poor health status is further aggravated by the subhuman conditions in the camps. Malnutrition rates for both women and children are close to emergency levels. Out of the 163,200 children below the age of five, only 24,500 children with Severe Acute Malnutrition have been admitted for treatment but more remain in need. Anaemia amongst children six-23 months (>50 percent) and stunting (low height for age) in children between zero-59 months (>40 percent) continue to remain major concerns.
Food shortage in the camps contributes to malnutrition and increases susceptibility to deficiency and disease, particularly for pregnant women and breastfeeding mothers. According to the 2018 Joint Response Plan (JRP) Report, 12,200 metric-tonnes of food is required every month to sustain the Rohingya population in Bangladesh, and Cox’s Bazar currently faces an annual food deficit of 50,000 metric-tonnes.
Gender-specific risks
Women and girls account for just over 52 percent of the population in the Rohingya camps in Bangladesh, and one in six families is headed by a single mother. Several factors lead to women not using WASH facilities even when they are available, primarily, the lack of safety and a sense of shame.
“Shame”
Like for any other displaced community, ‘shame’ plays an important role amongst Rohingya women since they are further marginalised even within the minority community. The unplanned nature of toilets and bathing spaces, without any thought to additional private spaces, discourage women from using them. Currently, a single toilet or bathing space caters to around 100 people, across age and gender. The poor infrastructure-to-people ratio causes long queues, which includes men, making it difficult for women to use them. Thus, many women prefer washing and urinating in their own limited space in the camp shelter. Social and cultural norms also play an important role, since Rohingya women still follow the purdah system. Going outside to use toilets requires them to dress appropriately, an onerous task that can be avoided by using their shelter space.
The community lacks proper knowledge about menstrual health, and menstruation is incorrectly associated with shame and uncleanliness. Rohingya women mostly use natural materials such as mud, leaves, dung or animal skins to manage their menstrual flow.This is despite the provision of menstrual hygiene products as part of their dignity kits, which they are unable to use due to uneasiness while changing or washing re-usable sanitary pads or cloths, or disposing of them in a private and hygienic manner in the same space used by men. Thus, the lack of access to water and personal latrines and the consequent increase in open defecation is putting women and children at increased risk of diseases.
Safety Issues
Due to the limited number of toilets and bathing spaces, as well as the lack of private spaces, many women and children are forced to bathe or defecate in the open. Even when women-only toilets are provided, they are often missing proper locks, making them unsafe.
Water collection also presents security risks. Women travel to a certain point to collect water from private tankers. However, these tankers operate at odd hours and usually create long queues, endangering the safety of Rohingya women.While some solar lampposts have been installed, there is insufficient street lighting. Theft and vandalism are rampant. There have also been reports of women and children being sexually harassed inside the camps.
Bangladesh government’s response
Bangladesh has been exemplary in accommodating the displaced Rohingyas. However, it struggles to provide adequately for the more than 900,000 of them, both in terms of sheer capacity and financial burden. News reports say that around 2,000 government officials are involved in the management of the camps at various levels, at an annual cost of US$15.24 million.This is a huge sum, considering that Bangladesh is a low-income economy with per capita annual GDP of about US$ 1,827.
To be sure, the mass entry of the Rohingyas has affected Bangladesh’s land and local resources. For instance, the massive destruction of forests to build camp settlements has resulted in the loss of biodiversity. Moreover, in the early stages of the influx, the unplanned and makeshift settlements built on hill slopes and forest lands have made the area vulnerable to landslides and other natural disasters.
The Bangladesh government—with help from international and national aid agencies—is attempting to improve the situation in the camps, especially in the areas of health and WASH. However, more help from the international community is required to mitigate the fund crunch and to increase manpower. The GoB, aided by 100 health partners—including 66 international NGOs, 39 national NGOs, eight UN agencies and one observer—is focusing on implementing various measures to combat the present health challenges in the settlements.
The health-sector partners are under the leadership of the Civil Surgeon’s Office of Cox’s Bazar, the Directorate General Health Services Coordination Centre and the World Health Organization (WHO), for better planning and implementation of a coordinated emergency response. The sector has adopted a three-tiered coordination structure at district, sub-district (upazila) and union levels to combat the current health issues.
There are 132 health posts and 32 primary health centres (PHCs) in the camps, of which 29 operate round the clock. More health facilities are being constructed and/or planned to meet the growing needs in the sector. The health partners also run field hospitals, diarrhoea treatment centres, specialised sexual reproductive health and/or delivery facilities, and other specialised health facilities (e.g. eye-care facilities, rehabilitation facilities, age-friendly centres and diphtheria-treatment centres). However, some of these specialised services are not widely available. In 2018, a number of vaccination programmes were launched to control the incidence of ARI, AWD and unexplained fevers, but these remain inadequate.
Registered Rohingyas receive more medical assistance than the unregistered ones,and it is imperative to avoid duplicity of services. Moreover, the distribution of health cards should not be contingent on registration.
To strengthen intersectoral collaborations, the health sector is working closely with the WASH sector by holding weekly meetings that focus on analysing the data available on WASH conditions and health risks. Such analyses yield evidence that facilitates on-ground discussions regarding contingency planning and disease control. The health sector is also working to identify priority camps for interventions and develop joint action plans.
The WASH sector, under the leadership of the Bangladeshi Department of Public Health Engineering (DPHE), is co-chaired by the United Nations Children’s Fund (UNICEF) and Action Against Hunger. The sector is tasked with the coordination, monitoring and strategic planning for WASH-related aspects across the humanitarian response.The earlier WASH interventions were mostly quantity driven, which led to the compromised quality of various infrastructure such as latrines, tube-wells and water pumps. The focus has now been shifted to the quality of infrastructure as well as strengthening operational management and community-based engagement.
Despite such efforts, the WASH sector still suffers from various gaps:
The JRP for the Rohingya Humanitarian Crisis remains underfunded. This was created by the UN, along with the UNHCR and the IOM, to provide support for the humanitarian response for the displaced Rohingyas. In the first JRP in 2017, funding of US$ 434 million was requested, of which only 64 percent was fulfilled. In the second JRP in 2018, US$ 950 million was requested and only 69 percent of it was received. Currently, only 14 percent of the US$ 920 million proposed in the third JRP (2019) has been supplied, out of which the WASH sector requires US$ 136 million.The health sector has only received 1.7 percent of its total requirement of US$88.8 million. Increased funding is thus crucial to strengthening the WASH and health sectors.
The international community has extended relief in the forms of direct service delivery of primary, secondary and specialised health facilities. They have established expansive community health worker networks and developed risk communication materials. Medical supplies are being delivered, vaccination campaigns held, and routine immunisations strengthened. There have been consistent efforts towards improving water quality in health facilities, capacity building of medical personnel; and preparation for disease outbreaks. Despite such fundamental efforts, however, financing remains a critical issue.
India’s involvement
India has the largest affordable and accessible public health service in South Asia. It has wide national-level programmes on communicable and non-communicable diseases. Further, India has provisions for providing counselling, testing and treatment—including certain social safeguards—and the resources to support community-based networks or interventions. Bangladesh and Myanmar are geopolitically important for India’s economic and political engagement in South and South East Asia, and the latter has close relations with both nations. Particular to the health sector, India has active bilateral health cooperation with the two nations.
In the context of the Rohingya crisis, India has strongly opposed the displaced community living in its territory, citing “national security” concerns. The recent ‘pushback’ approach of the BJP-led government towards the Rohingyas—i.e. sending them back to Myanmar—has created an uproar in the international circles and placed India in direct conflict with the UN. However, India is sympathetic towards displaced Rohingyas living in Bangladesh and Myanmar. According to the MoU signed in 2017 on Rakhine State Development Programme with Myanmar’s Ministry of Social Welfare, Relief and Resettlement, India pledged US$ 25 million for a five-year development project. Thus, India is constructing 250 houses for the displaced Rohingyas in the Rakhine state of Myanmar. President Ram Nath Kovind, during his visit to Myanmar in December 2018, handed over the first 50 houses towards this goal.
Similarly, India has extended assistance to Bangladesh under the umbrella of “Operation Insaniyat.” The relief material being provided has been divided into multiple consignments. Four tranches of relief materials have already been sent.
Given India’s better healthcare facilities and the dire situation of the camp areas in Cox’s Bazar, the former could assist Bangladesh further by aiding in the management of the public health situation in the camp areas. Under its “Aid to Bangladesh” programme, the Government of India is currently funding the construction of 36 community clinics in five northeastern districts of Bangladesh, namely, Sunamganj, Habiganj, Brahmanbaria, Jamalpur and Sherpur.Each community clinic is envisioned to cater to a population of about 6,000 and will provide primary healthcare, with emphasis on maternal and child healthcare services. The establishment of community clinics, especially in Habiganj (445.1 km) and Brahmanbaria (353.5 km), near Cox’s Bazar will help reduce the strain on Bangladesh. The infrastructure, medical and technical know-how from India can improve the coordination and functioning of the health programmes in Cox’s Bazar.
The following have been distributed under India’s “Operation Insaaniyat”:
Indeed, India and Bangladesh have come a long way in terms of mutual cooperation in various areas. The signing of the landmark Land Boundary Agreement in 2015 settled the longstanding border issues between the two. They have initiated joint patrolling across borders to intercept cross-border movement of insurgents, smuggling of narcotics and other transboundary crimes. The two countries are also strengthening their maritime relations.
However, India’s recent pushback against the Rohingyas has created a precarious environment. The fear of arrests and persecution has forced many Rohingyas, settled in India for generations, to escape and enter Bangladesh. This situation poses a threat to the equilibrium in India–Bangladesh ties, since the latter is already overburdened with hosting the Rohingya refugees. While India’s “Operation Insaniyat” has been successful, the country can consider extending more substantial support in the health sector. For instance, primary and secondary healthcare services need to be improved and made more accessible and geographically well-placed to target high-level trauma, communicable diseases and reproductive health needs. As discussed earlier, India is already constructing community clinics around Cox’s Bazar. However, the ones slated to be developed are still far away from the camp areas. Construction of community clinics close to the camps will benefit the displaced Rohingyas. Additionally, India can consider providing medical personnel to cater to the 900,000 Rohingyas in Bangladesh. Under Operation Insaniyat, India can also consider sending more relief items such as solar lamps, soaps, menstrual hygiene products, raincoats and umbrellas, which will be particularly necessary during the monsoon seasons.
The following are the most crucial and immediate requirements to improve the living conditions in the camps at Cox’s Bazar:
Conclusion
According to the World Health Organization, WASH is key to meeting the Millennium Development Goals related to environmental sustainability and good health. It is a priority sector that affects women and children more adversely than the rest. Unfortunately, quality WASH facilities, especially in maternity and primary-care settings, are absent in the Rohingya camps. Thus, a gender-focused approach is essential to alleviate the suffering of women and children, and achieve better sanitation and hygiene behaviour. Particularly during monsoon seasons, quality WASH systems are crucial, since there is an increased risk of diseases such as ARI and AWD.
The security concerns associated with the use of public latrines and bathing spaces can be mitigated by installing more solar street lights and increasing security personnel—particularly women—in the camps areas. Further, better law and order and proper investigation of gender-based crimes and vandalism are essential.
Bangladesh is an overpopulated country of more than 168 million people. This situation is worsened by the steadily growing number of displaced Rohingyas entering the region. To respond to this crisis in a humanitarian manner, financial assistance is vital. Unless international financial support increases, Bangladesh will have to bear a huge financial burden. While the international community does offer assistance, the amount currently committed is neither sufficient nor consistent. Moreover, aid agencies often contribute much less than they report, with funds being either mishandled or misused. Given the unreliable repatriation efforts by governments and agencies, the GoB has to consider other long-term solutions. The Rohingya crisis should be treated with the urgency that it demands. Integrated solutions—both at national and regional levels—are yet to be formulated and must emerge from within a formal policy framework in relief and healthcare.
The author is indebted to Dr. Anasua Basu Ray Chaudhury, Senior Fellow of ORF Kolkata, for her guidance and encouragement throughout the drafting of this article. She is also thankful to Dr. Ashish Banik of Bangladesh Enterprise Institute for his invaluable support.
Endnotes
[1], “de jure stateless” refers to a person who is stateless and therefore lacks membership to any basic institution (education, health care, employment) of the state and thus will be seen and treated as a foreigner by every country in the world. Source: Atig Ghosh, “Words of law, worlds of loss: the stateless people of the Indo-Bangladeshi enclaves”, in The State of Being Stateless: An Account of South Asia, Eds., Atig Ghosh, Anasua Basu Ray Chaudhury and Paula Banerjee (New Delhi: Orient Blackswan Publication, 2015), 20-49.
[1] “Culture, Context and Mental Health of Rohingya Refugees”, United Nations High Commissioner for Refugees, 2018.
[2] Ibid.
[3] “JRP for Rohingya Humanitarian Crisis, January – December”, UNHCR, February 2019.
[4] “Myanmar’s 1982 Citizenship Law and Rohingya”, A Briefing by the Burmese Rohingya Organisation UK (BROUK), December 2014.
[5] Brooten Lisa, “Blind Spots in Human Rights Coverage: Framing Violence Against the Rohingya in Myanmar/Burma,” Popular Communication 13 (2015): 132–14.
[6] Nehginpao Kipgen, “Conflict in Rakhine State in Myanmar: Rohingya Muslims’ Conundrum”, Journal of Muslim Minority Affairs, 2013, Volume 33, Issue 2.
[7] See Note 1.
[8] See Note 3.
[9] Submission by the UNHCR for the Office of the High Commissioner for Human Rights’ Compilation Report, Universal Periodic Review, Bangladesh, United Nations High Commissioner for Refugees, 2012.
[10] Ibid.
[11] The Foreigners Act, 1946, (ACT NO. XXXI OF 1946).
[12] See Note 1.
[13] Ibid.
[14] Ibid.
[15] Ibid.
[16] See Note 3.
[17] “The Rohingya Amongst Us: Bangladeshi Perspectives on the Rohingya Crisis Survey”, Xchange Foundation, 28 August 2018.
[18]Ibid.
[19] See Note 3.
[20] Abul Hasnat Milton, Mijanur Rahman, et al., “Trapped in Statelessness: Rohingya Refugees in Bangladesh”, Int. J. Environ. Res. Public Health 14, no. 8 (2017): 942.
[21] “World must not turn away from Rohingya crisis, say UN chiefs”, United Nations High Commissioner for Refugees, 26 April 2019.
[22] See Note 3.
[23] Ibid.
[24] Humayun Kabir Bhuiyan, “Rohingya repatriation: Myanmar to extend ‘secret’ MoU with UNHCR, UNDP for another year”, Dhaka Tribune, 6 May 2019.
[25] See Note 17.
[26] Situation Report Rohingya Refugee Crisis, Cox’s Bazar, Inter-Sector Coordination Group, January 2019.
[27] See Note 20.
[28] Dignity kit contains soaps, clothes, scarves, menstrual hygiene products and flashlights.
[29] “Bangladesh: Analysis of Gaps in the Protection of Rohingya Refugees”, UNHCR, May 2007.
[30] See Note 20.
[31] “Disaster Risk Management for Health Water, Sanitation and Hygiene”, WHO, UK Health Protection Agency and Partners, Global Platform, May 2011.
[32] Ibid.
[33] Victoria Palmer, “Analysing cultural proximity: Islamic Relief Worldwide and Rohingya refugees in Bangladesh”, Journal on Development in Practice 21, no. 1 (2011).
[34] “Rohingya Crisis in Cox’s Bazar District, Bangladesh: Health Sector Bulletin 9”, Health Sector Cox’s Bazar, May 2019.
[35] Ibid.
[36] Mohammad Mainul Islam and Tasmiah Nuzhath, “Health risks of Rohingya refugee population in Bangladesh: A call for global attention”, Journal of Global Health, The University of Edinburgh, 9 November 2018.
[37] See Note 26.
[38] “One year on time to put women and girls at the heart of the Rohingya response”, Oxfam, September 2018.
[39] Ibid.
[40] Shaheeda Kirtane, “Rohingya refugees under health crisis”, Expert Speak, Observer Research Foundation, 7 June 2018.
[41] See Note 34.
[42] Ibid.
[43] See Note 26
[44] Ibid.
[45] See Note 3.
[46] Ibid.
[47] Ibid.
[48] Ibid.
[49]REACH and UNICEF, “Water, Sanitation and Hygiene Assessment – Monsoon Follow-up”, Cox’s Bazar – Rohingya Refugee Response Report, October 2018.
[50] Ibid.
[51] Ibid.
[52] See Note 38.
[53] See Note 3.
[54] Ibid.
[55] “Signify and BRAC light the lives of over 46,000 Rohingya families in Bangladesh”, Reliefweb, 6 August 2018.
[56] “Rohingya refugees remain a heavy burden on Bangladesh”, The Conversation, 20 August 2018.
[57] “Bangladesh GDP per capita 1960-2019”, CEIC.
[58]“Rohingya Crisis in Cox’s Bazar District, Bangladesh: Health Sector Bulletin 9,”op. cit.
[59] Ibid.
[60] Ibid.
[61] Ibid.
[62] Ibid.
[63] See Note 3.
[64] “Rohingya Crisis in Cox’s Bazar District, Bangladesh: Health Sector Bulletin 9,” op. cit.
[65] See Note 56.
[66] See Note 3.
[67] Ibid.
[68]“Rohingya Crisis in Cox’s Bazar District, Bangladesh: Health Sector Bulletin 9,”op. cit.
[69] Joyeeta Bhattacharya, “Bangladesh first: Behind India’s changing stance on the Rohingya”, Commentaries, Observer Research Foundation, 23 May 2018.
[70] Sreeparna Banerjee, “Myanmar: India’s push-back approach towards Rohingyas”, South Asia Weekly, Observer Research Foundation, 24 January 2019.
[71] K. Yhome,“Examining India’s Stance on the Rohingya Crisis”, ORF Issue Brief, July 2018.
[72] Dipanjan Roy Chaudhury, “President Ram Nath Kovind hands over 50 houses in Myanmar’s Rakhine state amid China’s growing presence”, The Economic Times, 11 December 2018.
[73] “Operation Insaniyat: Humanitarian assistance to Bangladesh on account of influx of refugees”, Ministry of External Affairs, Government of India, 14 September 2017.
[74] “First Community Clinic with Government of India funding, at Chechan, Chhatak, Sunamganj District”, The Asian Mail, 5 February 2018.
[75] See Note 75.
[76] Zarir Hussain, “India deports second Rohingya group to Myanmar, more expulsions likely”, Reuters, 3 January 2019.
[77] Sreeparna Banerjee, “Myanmar: India’s push-back approach towards Rohingyas”, South Asia Weekly, Observer Research Foundation, 24 January 2019.
[78] Ibid.
[79] See Note 38.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Sreeparna Banerjee is an Associate Fellow in the Strategic Studies Programme. Her work focuses on the geopolitical and strategic affairs concerning two Southeast Asian countries, namely ...
Read More +