-
CENTRES
Progammes & Centres
Location
 PDF Download
PDF Download 
Ravi Mittal and Oommen C Kurian, “Bringing the Covid-19 Vaccine to Every Hamlet: The Story of Raigarh,” ORF Special Report No. 192, June 2022, Observer Research Foundation.
Introduction
In May 2022, the World Health Organization (WHO) reported that about 81 percent of the population of Africa were yet to receive a single dose of Covid-19 vaccine.[1] The story is different for India: Proving many earlier predictions wrong, and remarkably leveraging its domestic manufacturing capacity, India was able to roll out its vaccination effort quicker than most countries in the developing world. It managed to fully vaccinate almost 70 percent of the total population,[a] although there are variations in coverage across states.[2]
India launched its ambitious Covid-19 vaccination drive on 16 January 2021 with the aim of reaching 30 million healthcare and frontline workers. On 1 March 2021, the country initiated the second phase for those above-45 with comorbidities and the cohort above 60. This was expanded on 1 April 2021 to cover everyone above 45 years, bringing the total target to over 300 million people. While this number accounted for only 22 percent of the population, they were also high-risk and most vulnerable, accounting for 80 percent of recorded Covid mortality in the country at the time. During the devastating wave in April 2021, the sudden rise in cases and deaths compelled the Indian government to announce the third phase of its vaccination campaign: Beginning 1 May 2021, those above 18 years were inoculated, adding another 600 million people to the list.
Graph 1: Global Vaccination Coverage and India’s Impact on the LMIC Average
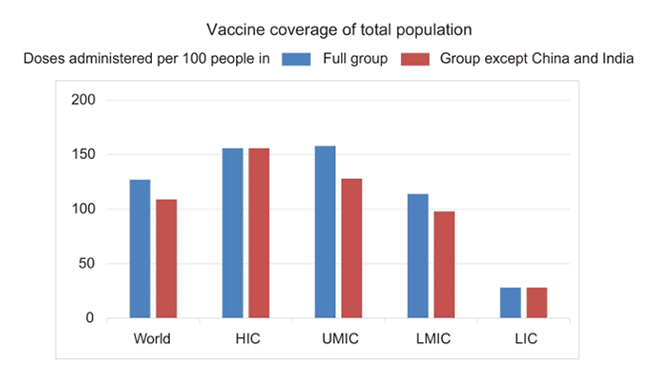
As of 6 June 2022, more than one billion Indians have received at least one dose, and 944 million are fully vaccinated. Full-vaccination coverage is higher in the 45+ population, at 95 percent. Indeed, among comparable lower- and middle-income countries (LMICs), India has one of the highest proportions of population vaccinated, as seen in Graph 1, which explores the huge impact of India’s numbers on the LMIC average. To be sure, however, there are stark differences in the coverage across states. Earlier during the drive, a slowdown in the pace of vaccination amidst the relatively low case and death numbers and the overall public impression of low risk, prompted a meeting of chief ministers. The ‘Har Ghar Dastak’ approach was launched, and the inoculation campaign managed to pick up pace again.
Map 1: Coverage of Second Doses Across Indian States
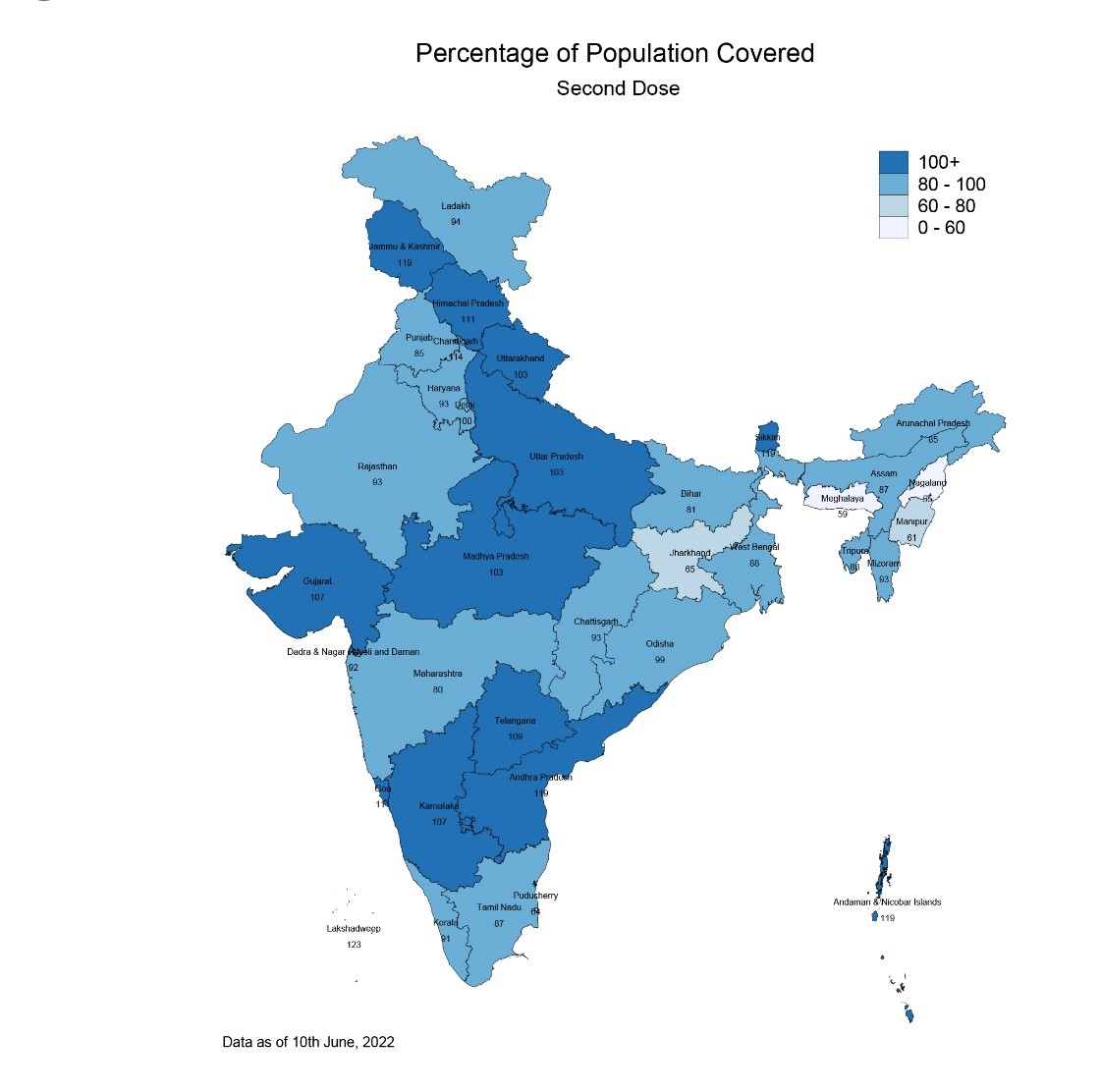
While some Indian states are still lagging in universal vaccination, there have been many notable achievements: the Covid-19 vaccination drive has been conducted at an exceptionally fast pace in most Indian states, and near-universal coverage has been ensured, even within some of the low-income Empowered Action Group (EAG) States.
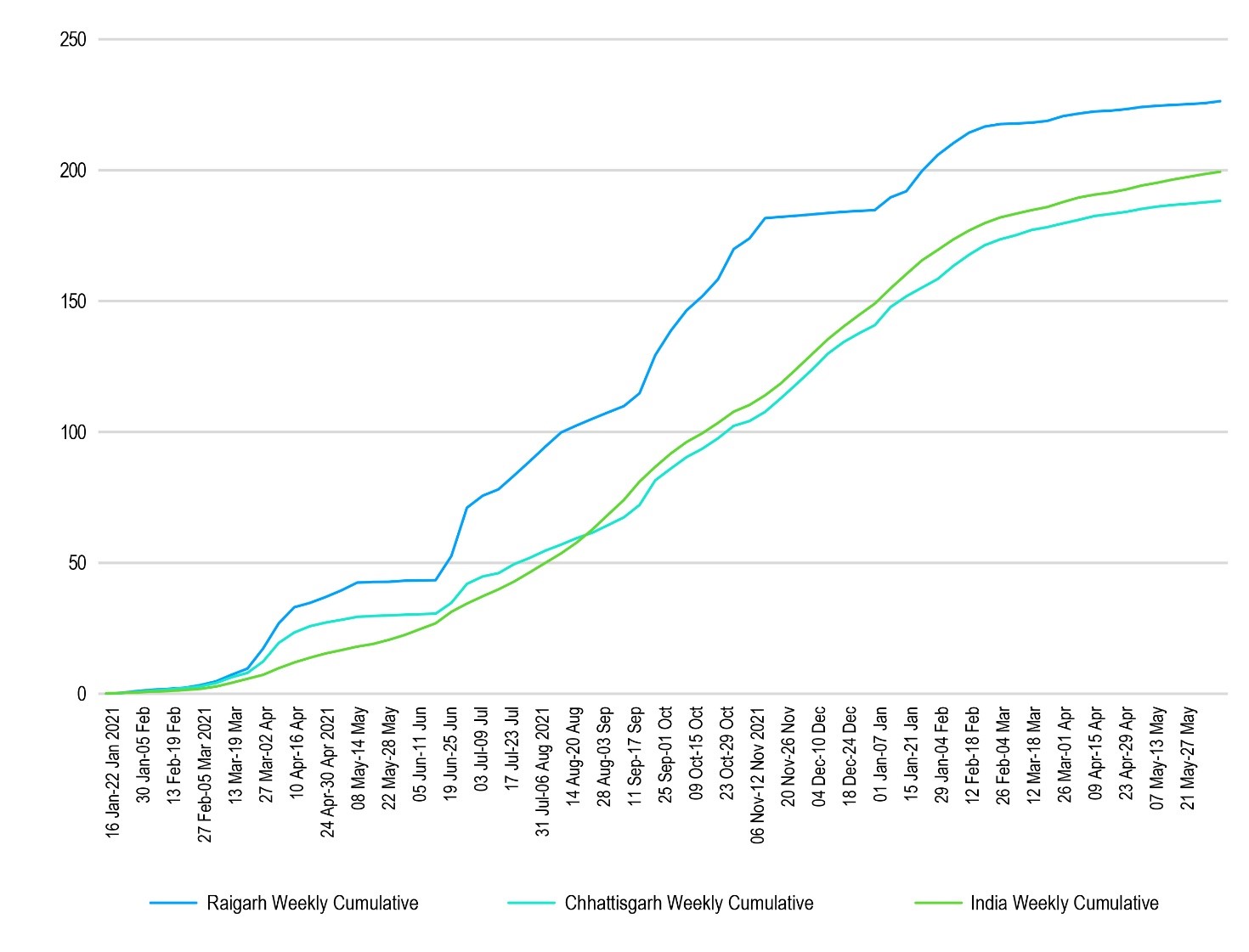
In the state of Chhattisgarh, for example, by 9 November 2021—i.e., just 298 days after the vaccination campaign started, the district of Raigarh had reached its target of vaccinating all adult citizens with the second dose. At that time, the national achievement was a far lower 35 percent of the target population fully vaccinated, and over 77 percent with a single dose. (Graph 2 tracks the timelines for Raigarh, Chhattisgarh, and India overall.) While Chhattisgarh’s number of cumulative doses per 100 adult population has stayed close to the national average throughout the vaccination drive, Raigarh accelerated early on, and kept its pace.
Graph 2: Vaccination Timeline: Raigarh, Chhattisgarh, and India
Upon reaching 100-percent full vaccination coverage in November 2021, Raigarh—with a population of 14.94 lakhs according to Census 2011—became one of the first districts in India to achieve vaccination for all. Scheduled Castes (Dalits) comprise 15 percent of its population, and Scheduled Tribes (Adivasis), 34 percent. There is a considerable population of Particularly Vulnerable Tribal Groups (PVTGs) in the northernmost hilly part of the district.
This report identifies the factors for the success of Raigarh’s vaccination campaign. With full vaccination in regions like Africa still under 15 percent, this experience of success from a region known for its low income and weak health infrastructure could offer lessons for the rest of the world. These lessons can be particularly useful given the emerging vaccine fatigue with respect to booster shots.[3]
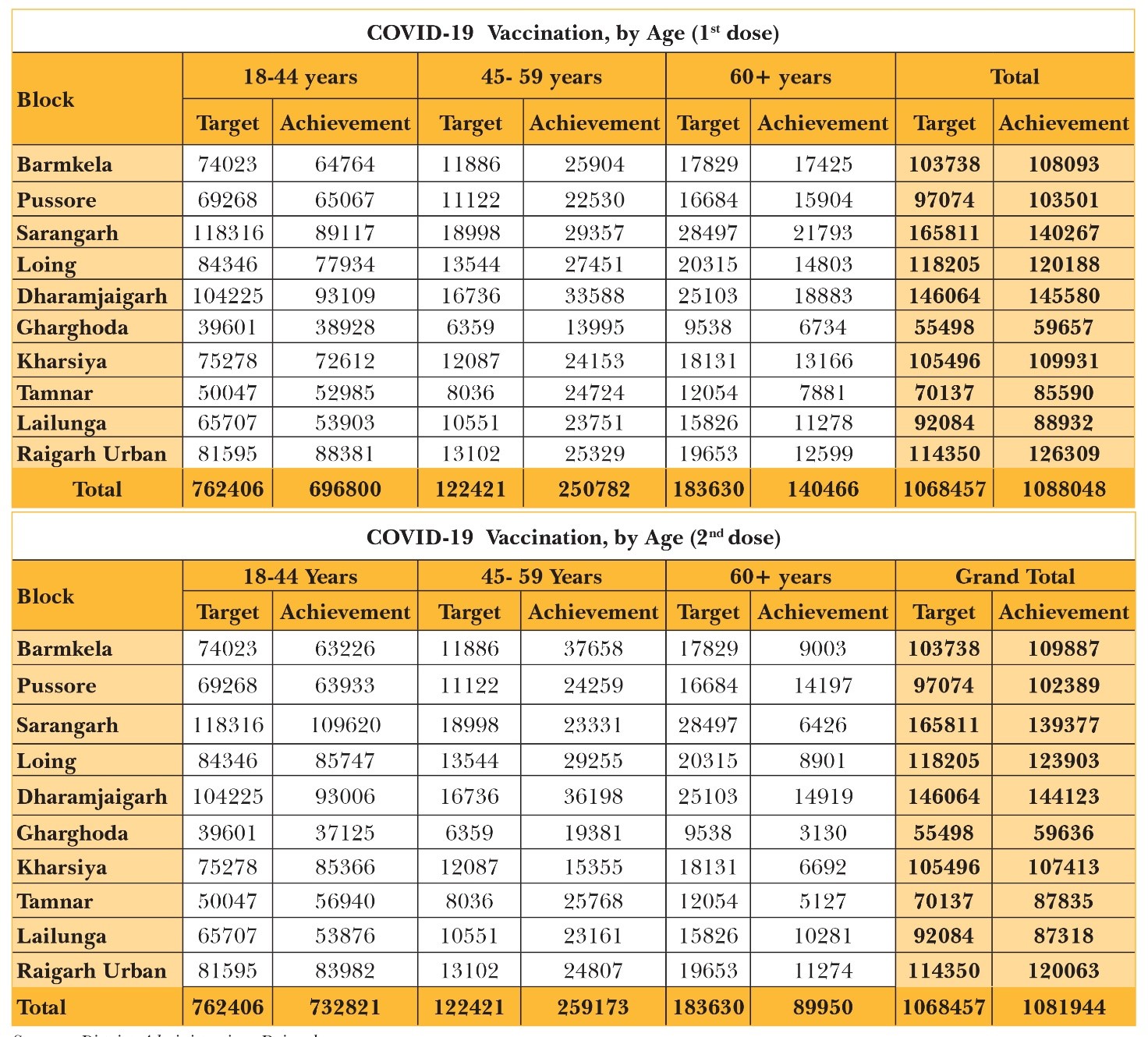
Indeed, during its early phases, Raigarh’s vaccine rollout for the elderly moved slowly for reasons such as difficulty in reaching the sites due to immobility, and severe illness. Moreover, the projected target population estimated for the elderly— based on an extrapolation of the 2011 census—did not match the actual field survey conducted in the Gram Panchayats and the urban wards. Therefore, there was a gap in vaccination for the 60+ cohort between actual achievement and estimated targets. The inadequacy of age-specific population estimates for planning became evident, as the actual vaccination numbers for the 45-59 age category proved to be almost double the projected target. The absence of reliable age-disaggregated data on the population led to such differences.
Table 1: Vaccination Targets Vs. Achievements in Raigarh, by Block (November 2021)
Raigarh’s Vaccination Drive: The Initial Phases
Other nationwide campaigns, such as elections for instance, are hardly able to achieve 100-percent coverage. The challenge was more formidable for the life-saving Covid-19 vaccination drive. To begin with, the timeline to accomplish the task was unprecedented in India. Furthermore, many sectors and government entities had then only started to recover from the devastating two waves when the vaccination gained momentum. The government machinery was required to clear the pre-pandemic backlogs, requiring extraordinary effort. Thus, the inoculation campaign could only expect limited support from other departments, such as those of Women and Child Development as well as Rural Development, which both play integral supportive roles in the activities of the health department.
In Raigarh, the vaccination campaign was not without challenges: some of these difficulties were foreseen, similar to those faced in other campaigns, and mere reflections of national and state-level challenges; however, many other obstacles were unexpected, were unique to the Covid-19 situation, and were peculiar to the district. These varied challenges can be broadly classified as structural and functional.
Foremost among the structural challenges was vaccine shortages. Issues with the development, production, and distribution of the vaccines resulted in irregular supplies, and the frequent shortages resulted in uncertainty. Moreover, regular changes in policy required a strategy that needed to keep all the stakeholders abreast with the latest developments. For instance, the phased rollout beginning with the healthcare workers to frontline workers, to the elderly with comorbidities, and so on, required innovative strategies for mobilising the targeted cohorts in a timely manner. Similarly, the shift of vaccine procurement responsibilities to the states and the subsequent reversal to central procurement, impacted the focus on beneficiary targeting.[4] Third, resource limitations within the health system made it a daunting task to sustain the pace of the campaign while maintaining the essential health and routine immunisation services. Both human resources—i.e., vaccinators, operators, drivers—and the physical resources such as the venues for vaccination and vehicles for transport, were limited. As confidence towards the vaccine improved with new evidence, norms were gradually relaxed, aiding in the efficient deployment of resources.[5]
In parallel, many functional challenges were recognised early during the pilot vaccination of healthcare and frontline workers. The most prominent was vaccine hesitancy, varying degrees of which were seen in different populations. For instance, blue-collar workers were concerned about potential loss of wage, not only for the particular day they would need to travel to the vaccination site but also in the event that they develop a fever following the jab. The hesitancy can also be explained as a result of fear-mongering rumours on social media, and safety concerns especially in areas where individuals have been reported to have experienced adverse side-effects from the inoculation.
Yet, there were pockets in the district that showed vaccine eagerness, leading to turn-outs higher than expected and, consequently, vaccine shortages. Raigarh, in the easternmost part of Chhattisgarh, is home to a considerable tribal population and access challenges proved to be daunting. Geographically, the district varies from thinly populated remote tribal hamlets in the forest-covered plateau in the north, to the densely populated treeless plains in the middle and south. There were unique challenges, therefore, among them unexpected power outages, and poor road and internet connectivity in forested remote areas. Moreover, the district is mainly rural and agricultural, albeit with a rapidly growing industry sector. The large number of floating populations posed a unique challenge. Despite regular updates in the COWIN portal, technical issues were frequently encountered by the field staff.
Initiatives taken up at the national and state levels gave impetus to the district campaign in Raigarh. These include mandating mobile service providers to ensure vaccination caller tunes, and social media campaigns. The massive second Covid-19 wave could also have acted as a natural catalyst by showing examples of how the vaccinated healthcare and frontline workers were least affected by the Delta surge.
The time-bound vaccination rollout required detailed planning to ensure safety as well. The set of challenges were overcome with a coherent and meaningful strategy, which involved bottom-up planning. The District and Block Task Force committees, led by the District Collector and SDMs, respectively, ensured preparedness even before the start of the campaign. Set up in late 2020, these committees provided a platform for cooperation and collaboration between stakeholders, and identification of bottlenecks and challenges at all levels. For instance, with the limited availability of vaccines during the initial phase, the planning and coordination for adequate security arrangements with the police department were carried out in these meetings. Subsequently, they provided closed monitoring and supervision of the campaign.[6]
The adversities were turned into opportunities. For instance, officials utilised the time during vaccine scarcity to update surveys on the vaccination coverage, formulate the vaccination plans for different areas, and carry out motivation strategies. Moreover, cues were taken from the experience of implementing other programmes and campaigns such as management of elections, as well as Information, Education and Communication (IEC) campaigns taken up under the Swacch Bharat Mission (SBM).
Raigarh’s Strategies
In Raigarh, the challenges faced by the vaccination drive were overcome by systematic participatory strategies, underlined by building trust among various stakeholders. As Nobel Prize-winning economist Kenneth Arrow once said, “Trust is an important lubricant of a social system.”[7] To nurture trust within the community, it is crucial to engage all stakeholders through collaboration.
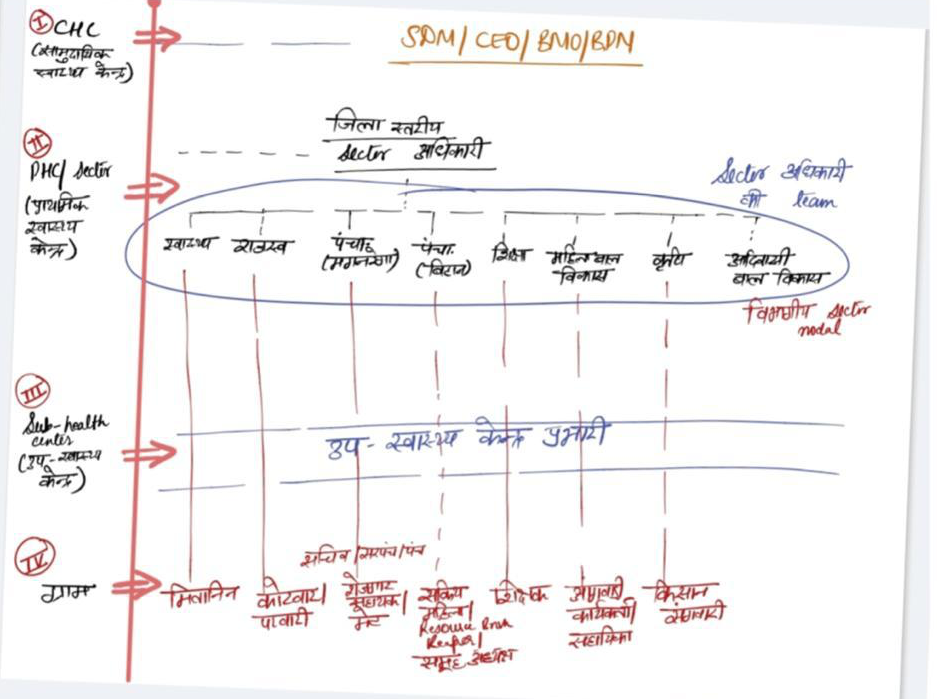
Engaging all stakeholders. Local-level public representatives and government officials were amongst the first to be approached. Studies have found that in developing societies, households accord greater trust in government; this is especially true for poor and disadvantaged families.[8] Moreover, by representing diverse communities, they can effectively influence and mobilise the people by acting as direct sources of information. For instance, Panchayati Raj Institutions (PRIs) played a remarkable role during the severe months of the pandemic by providing essential leadership at the local level.[9] The district administration leveraged this trust by engaging public representatives and officials from different departments. The public representatives at the grassroots, especially Sarpanch and Panches in the villages and ward members in the urban areas, were actively involved through physical and virtual meetings.
Furthermore, local-level officials from different departments acted as local influencers. These officials included ASHAs, Anganwadi workers, Gram Panchayat Secretaries, teachers, farmers’ friends, and Kotwars and Patels.[10] Such an engagement of public representatives and officials was a key to building confidence.
Leveraging various social networks. Research shows that it is crucial to capitalise on the creditworthiness of social networks to disseminate information.[11] In many Asian societies, individual preferences are shaped by those of specific others, especially people they trust and respect.[12] Therefore, local elements of social capital facilitate citizen participation.[13] At all stages of the campaign, the Raigarh administration actively engaged networks such as self-help groups (SHGs), Mahila Arogya Samitis, religious institutions, volunteer organisations, youth networks such as NYK, NSS & NCC, NGOs, and village elders.
Aligning stakeholders’ interests with the campaign objectives. The interests of other stakeholders were aligned for mutual benefit through creative strategies. For example, business establishments provided discounts, and in the urban areas, eco-clubs distributed free saplings upon presentation of vaccination certificates. Development partners such as UNICEF and Azim Premji Foundation also played a remarkable role at different stages of the campaign.
Optimising resources. The vaccination campaign presented the twin challenges of vaccinating all the citizens at an unprecedented scale and speed, while ensuring essential health services. Therefore, resource mapping, planning and optimisation were crucial for effective and efficient allocation of resources. First, the state health department mapped healthcare workers who can potentially support the vaccination effort with desired skillsets working both in the government and private sector, as well as those currently not employed or are retired. They included frontline personnel and back-room support staff, including vaccinators, verifiers or data entry operators, mobilisers, and crowd managers. The budgetary support for operational costs allowed their engagement, whenever required.
From the beginning, it was evident that the campaign would be a marathon, not a sprint.[14] Therefore, it was critical to prevent burnout amongst the staff. An effective rotation policy was designed to ensure adequate rest and the continuity of routine health services as well as a scaled-up vaccination campaign even during weekends. Moreover, context-specific solutions were devised for the effective utilisation of human resources. For instance, centralised entry of records was done in some blocks to minimise the requirement of on-ground data entry operators. Along with human resources, a parallel mapping of physical health infrastructure was planned and carried out, with the aim of optimally placing Covid-19 vaccination centres. These included community halls, schools, Resident Welfare Association (RWA)-designated spaces, industrial premises, and other government and private sector spaces.
Devising the distribution plans. Due to frequent vaccine shortages, it was essential to have an objective allocation plan. Therefore, the blocks were allocated vaccines based on the principle of ‘Vaccinate more, Get more’. Apart from motivating better performance, it ensured the optimal distribution of scarce resource. Moreover, the plan utilised lessons from both the management of routine immunisation campaigns and elections in India. For instance, route charts were drawn to ensure that vaccines, first-aid kits, and other materials are delivered to multiple sites in the shortest possible time and using the least possible number of vehicles.
Regular engagement with the frontline personnel. This made sure that correct information and strategic priorities were passed on to the lower rungs of the healthcare ecosystem. Frequent national and state-level policy shifts necessitated the regular training of personnel at all levels. Innovative strategies were adopted to keep the stakeholders updated and resolve their concerns.[15] Therefore, a team of “master trainers” was nurtured, who posted short video messages on social media groups and managed helplines to resolve issues in real-time. Such measures allowed swift dissemination of information and built confidence among the workers.
Targeted Plan for Mobilisation
There is an aphorism that describes India well: “The language spoken in India changes every few kilometres, just like the taste of the water.”[16] Yet, the challenges in mobilisation are not only linguistic, but also ethnic, social, and religious. The wide range of density and geography— from thinly populated hamlets to dense cities and hilly terrains—compound the challenge. A targeted approach through bottom-up planning provided solutions.
The process started with defining the baseline. Vaccination targets for the districts are based on the population projected for 2021. Sixty-five percent of this projected population are adults. Since it is only an estimated target, the expected achievement will not precisely be 100 percent.[17] Within Raigarh, there are blocks that showed more than 100-percent vaccination coverage for this reason. Therefore, targeted planning using the district-level projected estimates will be imprecise and only approximate. It is thus critical to provide the actual workable figures for the blocks, urban bodies or villages and even rural and urban wards. To ensure this, the district utilised the electoral voter roll as baseline, the most popular and readily available database at the district level. The progress was regularly updated in this database by the field-level functionaries based on actual achievement.
Defining the electoral roll as the baseline provided the starting point for targeted planning by defining near-exact targets up to the grassroots level. Second, regular updates tracked the changes in demographics due to in and out-migration, marriages, and deaths. Third, it provided real-time data to identify the pockets with low coverage. It allowed focused review and interventions in such areas, for instance, extensive motivation campaigns in case of high vaccine hesitancy.
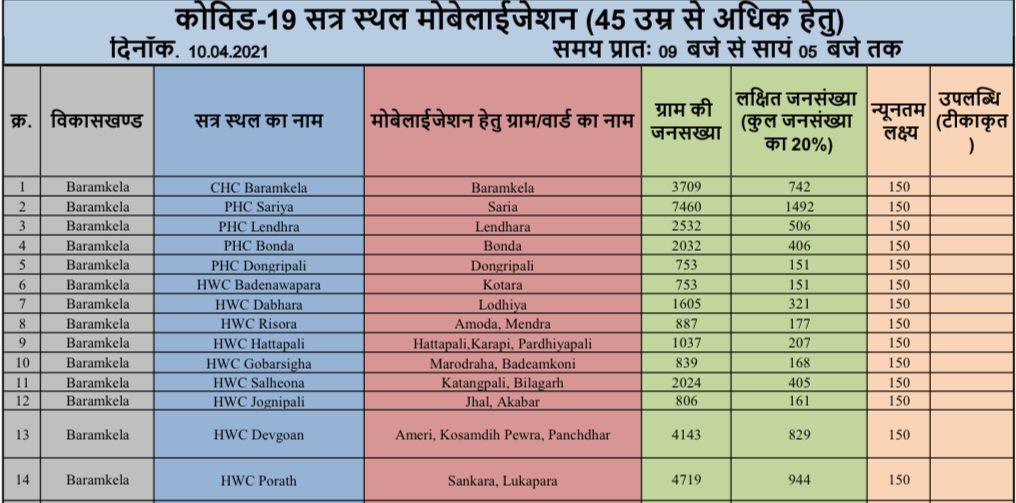
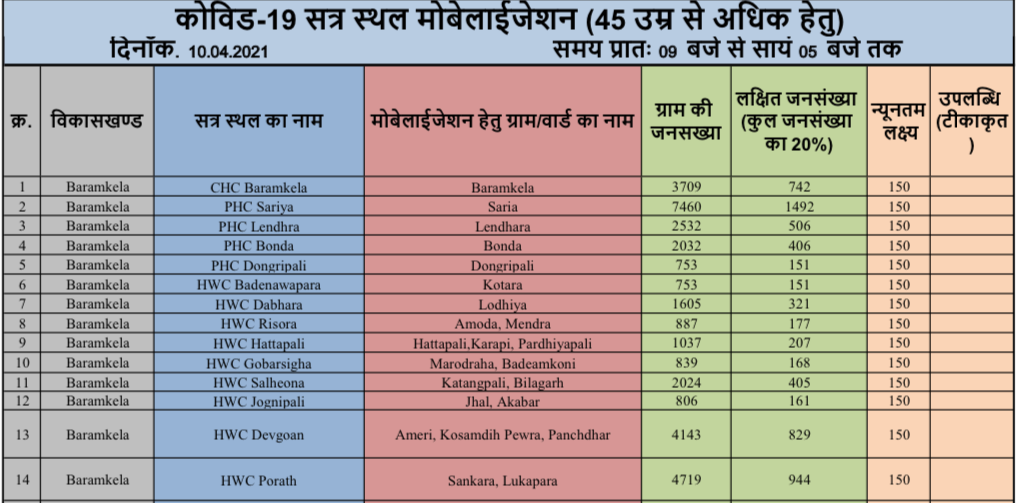
Formulating the Mobilisation Plans was the next step. Management of elections where polling booths are set up akin to the vaccination sites provided key lessons in devising the targeted strategy for vaccination. As a result, the district team formulated mobilisation plans through the bottom-up approach for targeted mobilisation. First, the blocks planned the number of vaccination sites and set the target for each. It was based on the availability of resources such as vaccinators and vaccines. Second, each site was linked with urban ward(s) or village(s) based on the remaining population numbers to be vaccinated in the target area. Third, the site plans of all the blocks were aggregated to form the district-level mobilisation plan. Finally, the district plan was circulated among all the stakeholders a few days before the actual date. It allowed ample time for planning the logistics and implementing the motivation strategies.
Figure 1: Decentralised Targets for Vaccination
The above planning paradigm was replicated every day. This targeted and astute planning with multi-stakeholder involvement engendered a festival-like spirit on the days of vaccination within the community.
At the outset, it was decided that a one-size-fits all approach would not be feasible for large diverse populations.[18] The focus was on devising context-specific strategies. Locating vaccination sites close to the people’s place of work or residence contributed to the higher vaccination rates. There were evening sessions for farmers who work in fields during the day, mobile sessions in urban places with high footfalls, and special camps for industrial workers within their work premises. Finally, community spaces within the villages were utilised for the door-to-door individual and community-focused vaccination campaigns. By providing convenience, the immunisation of the disadvantaged and reluctant communities was ensured.
In the course of the campaign, reaching and motivating populations in the far-flung areas and addressing vaccine hesitancy in pockets proved to be formidable challenges. On 23 July 2021, after two months of consistent efforts, the administration finally convinced a reluctant community in the village Bhikampura in Baramkela block to get the jab. Similarly, Santosh Ghosh, a vaccinator posted in the remote tribal area of the district, trekked several kilometres to reach the Pahadi Korva community, stayed there through the night, and returned only after ensuring complete vaccination. There is no dearth in stories of turnarounds and extraordinary efforts of healthcare workers who went beyond their call of duty. To motivate the community and the workers, multiple indigenous strategies were adopted.
The message, the medium and the messenger are crucial. The influential ‘messengers’ in the local ‘medium’ present a powerful ‘message’ to the community. Therefore, the campaign extensively used slogans, anecdotes, and jingles by famous artists and opinion-makers in the local languages. They were propagated through loudspeakers on bicycles, mobile marketing vehicles locally called ‘Tikakaran Rath’ playing jingles, wall writings, posters, and the local media. The regular dissemination of the clear message also dispelled myths about vaccination.
Furthermore, virtual conferences were held to provide a platform for the exchange of experiences and ideas. During such interactions, local representatives, healthcare and other local officials from the high-performing localities shared the motivation methods, which connect easily with the local population. Thus, it provided vital clues to the low performers on counselling and spreading the positive message. Focus was given to areas that suffered incidents of adverse side-effects.
During uncertain situations, people look to their leaders for cues. The various stakeholders, particularly government representatives, officials and reputed members of local-level social networks, are seen as torchbearers within their community. In the beginning, they, along with their family members, were motivated to get vaccinated. It set an example for others. Subsequently, the videos of these influential people were circulated in local social media groups, creating a high positive impact within the community.
Once the narrative is crafted and examples are set, it is essential to break the public inertia. The district organised a massive vaccination campaign on 26 June 2021. Additional resources were mobilised during the huge drive, and each district officer was allotted a sector to supervise all the campaign-related activities on that day.
Figure 2: Plan to Deputise Grassroots Workers at the Mega-Vaccination Campaign
The campaign was a success both in the short and long term. Immediately, 14 percent of the target population were vaccinated in a day, against the target of 5 percent. The long-term impact was that it converted ‘fear of unknown’ into ‘fear of missing out’, and filled the citizens with enthusiasm and eased further mobilisation.
The district administration widely recognised the public representatives of local self-governments, health workers, and other stakeholders of 100-percent vaccinated village(s)/ward(s) as champions.[19] Their success was celebrated through press releases, certificates of appreciation, and recognition during virtual meetings. It helped to motivate others and sustain the momentum.
This system ensured that the campaign did not lose steam midway. “What gets measured gets done” may be a cliché, but there is a reason it is. Regular monitoring was crucial to ensure effectiveness and correct the course whenever and wherever required.
This laid the foundation for the monitoring system. The first step was to define the intermediate and final outcome indicators. For example, percentage population coverage with daily progress was monitored both by block and village. Similarly, the average vaccination per session site reflected the efficiency and relevance of each site.
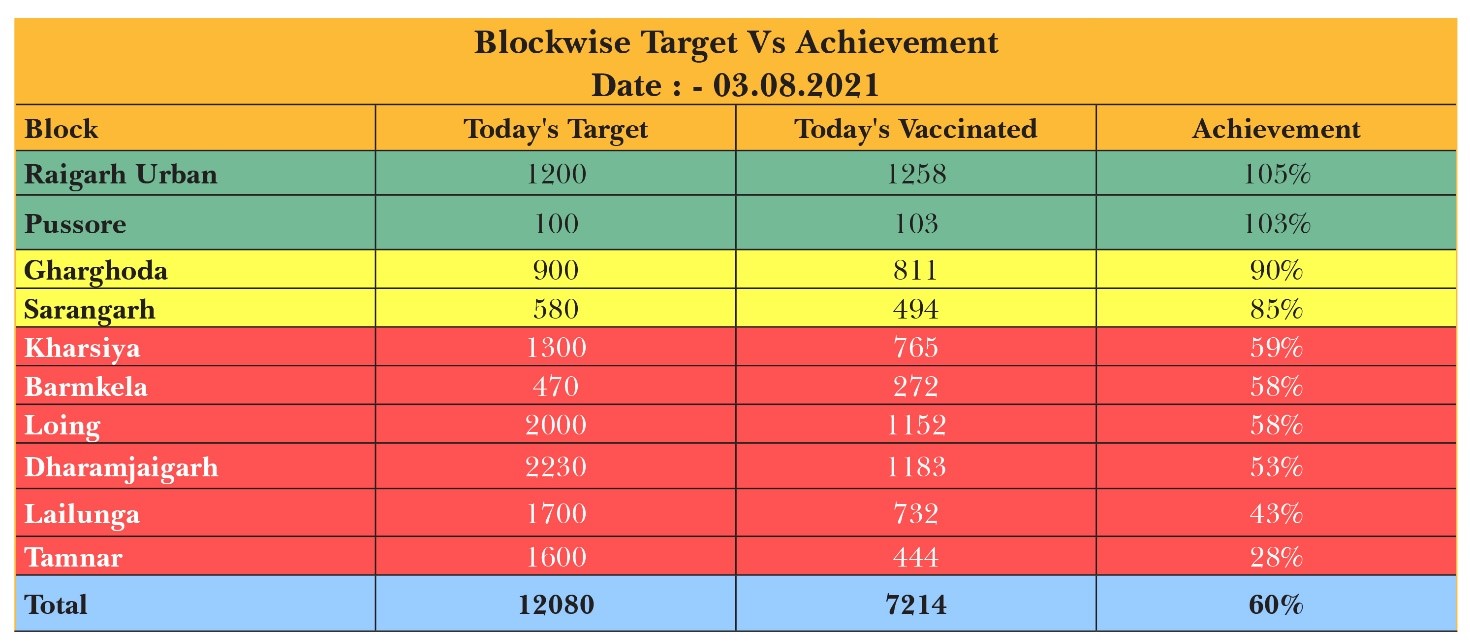
It is often seen that leveraging the elements of competitive play can unleash passion, potential, and personal commitment.[20] Therefore, gamification was introduced to the monitoring reports. The overall performance was sorted in a descending manner and arranged in the form of leaderboards. At the same time, the best daily performances were recognised with incentives like badges. The positions were colour-coded and the coded tables were posted in the official groups. It ensured the desired attention of the low performers to get out of the red zone.
Table 2: Block-Level Daily Performance Tracking
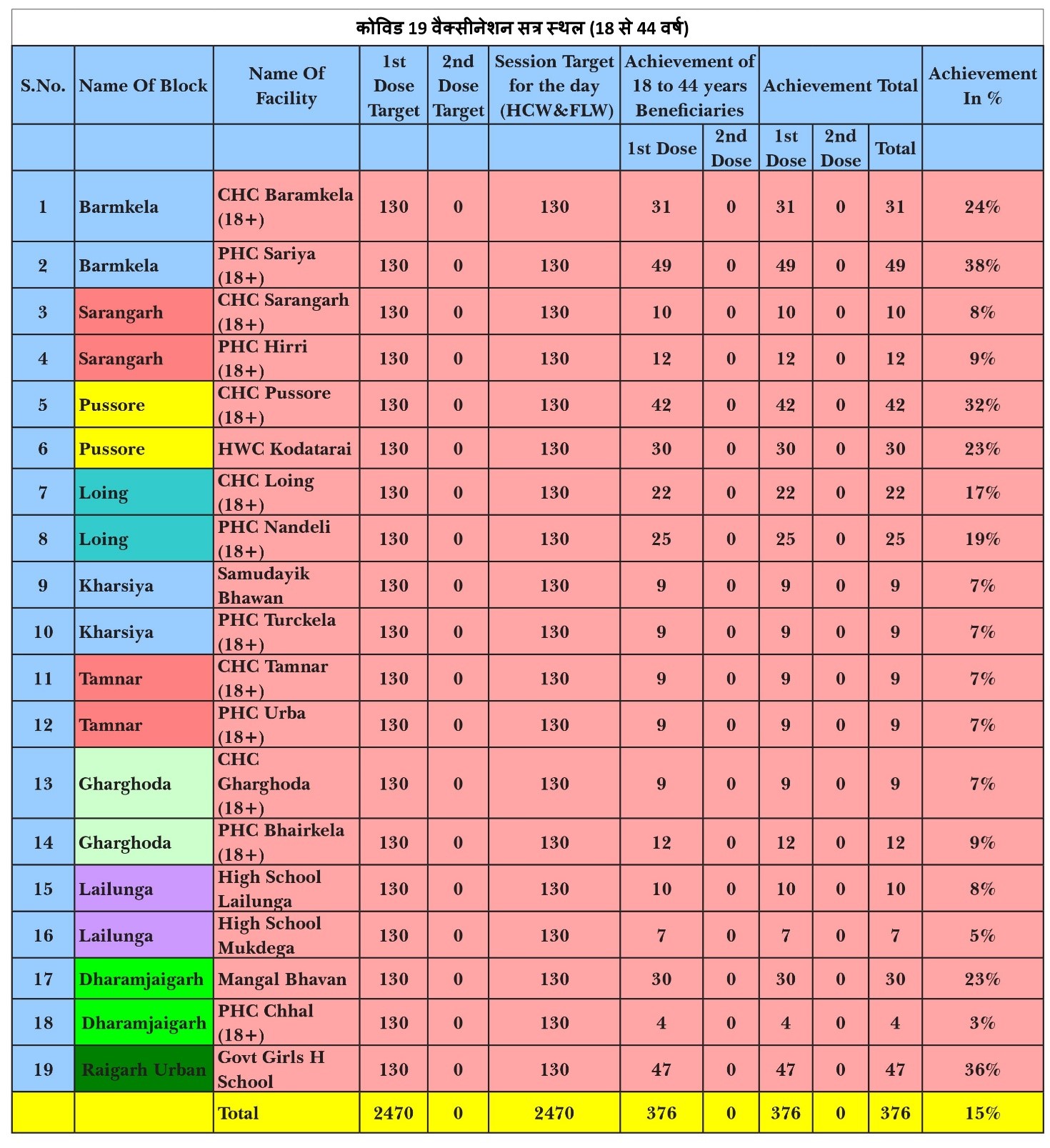
Besides giving impetus to the efforts of all the stakeholders, regular monitoring provides an opportunity for course correction. For instance, the achievement of each session site was monitored four times during the day, i.e. 11 AM, 1 PM, 3 PM & 5 PM through the Google Sheet (Figure 4). The vaccination team at sites with below-par performance during early hours were individually contacted. It helped solve many problems in real time. For example, making alternative arrangements in case of a team member’s uninformed absence or sending additional doses in case of unexpected high turn-out.
Table 3: Vaccination Sites with Poor Achievement at 1:00 PM on 02-05-2021
Regular monitoring through outcome indicators allowed continuous improvement in overall planning, improving efficiency. For example, the sites where the performance was consistently poor as shown by the poor average vaccination per site were individually evaluated. In some cases, they were found to be distant from the neighbourhood and thus, shifting the site to another building close to the community significantly improved the performance.
Conclusion
Raigarh’s success in taking the vaccination campaign to every hamlet is testimony to the multiple strengths of Indian democracy, including collaborative and cooperative federalism, the power of grassroots and civil society, and the value of unity in diversity. These lessons will go far beyond the Covid-19 vaccination campaign. The wisdom gained during the campaign will have a lasting impact on government institutions’ ability to implement large-scale social welfare measures. The unprecedented challenge of scale, scope, and speed will leave a long-lasting institutional memory. Therefore, it is an opportune time to contextualise the lessons from this experience for other policy measures in a granular manner.
The Raigarh experience shows that a collaborative approach, sustained commitment, and contextualised planning can help achieve goals, despite challenges at different points. At the grassroots level, the cross-pollination of ideas between multi-stakeholders such as ANM, ASHA, Gram Panchayat Secretary defined the problem-solving approach. The lessons from one village/ward or block held wisdom for the other struggling village/ward. Although different situations require a context-specific approach to problem-solving, this basket of challenges has relevance to diverse conditions. Therefore, it provides vital lessons for other districts—and cities, states, and even nations—on the mission to vaccinate citizens, particularly as many regions have only started overcoming supply constraints of vaccine doses.
Streamlining weak health infrastructure, overcoming gaps of health workforce, convincing a skeptical population, ensuring motivation amongst the workforce till population coverage is achieved, will be the predominant concerns for many such countries and regions going forward. It is very similar to where Raigarh was in early 2021 when the district flagged off its Covid-19 vaccination campaign.
Dr Ravi Mittal is an Indian Administrative Services (IAS) officer currently posted as the Chief Executive Officer of the District Panchayat in Raipur, Chhattisgarh.
Oommen C Kurian is Senior Fellow and Head of ORF’s Health Initiative.
The authors would like to thank Anshika Sharma for research assistance.
Endnotes
[a] More than one-fourth (26 percent) of Indians are under 15 years of age.
[1] World Health Organisation, “COVID-19 Vaccination in the African Region,” May 8, 2022, https://apps.who.int/iris/bitstream/handle/10665/354270/CV-20220513-eng.pdf
[2] “COVID-19 Vaccination Watch,” The Global Vaccination Campaign, Observer Research Foundation, 2022, https://www.orfonline.org/vaccine-tracker/
[3] “Vaccine Fatigue? Complacency, confusion, fear behind reluctance to take COVID booster, say experts,” Economic Times, April 26, 2022.
[4]In between, when the responsibility of procurement shifted to the states, Chhattisgarh drew its own priorities. e.g. – only Antyodaya Ration Card holders were initially considered. Then, the High Court intervened and a ratio for Antyodaya, BPL and APL card holders was fixed. Subsequently, when Central government rolled back the decision, vaccination was done as per the GoI mandate.
[5] Initially, the physical norms for the vaccination site such as number of rooms required and the number of members in the team were followed rigidly. Gradually, as confidence improved, the effort could be attempted even in places with lesser infrastructural facilities (number of rooms, for example) and with a smaller team.
[6] Bhim Singh and Ravi Mittal, “Raigarh instilled FOMO in people. That’s how it became a fully vaccinated district,” The Print, November 19, 2021, https://theprint.in/opinion/raigarh-instilled-fomo-in-people-thats-how-it-became-a-fully-vaccinated-district/767943/
[7] Harvey S James Jr., “On the Reliability of Trusting,” Rationality and Society, May 2002 https://ideas.repec.org/a/sae/ratsoc/v14y2002i2p229-256.html
[8] Deepak Kumar, Bhanu Pratap and Archana Aggarwal, “Public trust in state governments in India: Who are more confident and what makes them more confident about the government?,” Asian Journal of Comparative Politics, February 7, 2020, https://doi.org/10.1177/2057891119898763
[9] “Stronger at the grassroots,” The Hindu, October 8, 2021, https://www.thehindu.com/opinion/op-ed/stronger-at-the-grassroots/article36884992.ece
[10] Patel and Kotwar are people appointed from within the village to assist the administration in various panchayat-related tasks, especially involving land revenue. They are paid honorarium.
[11] Fukuyama, Francis. “Social Capital and Development: The Coming Agenda,” SAIS Review, January 2002, https://www.researchgate.net/publication/236762740_Social_Capital_and_Development_The_Coming_Agenda
[12] Iyengar, Sheena S. and Lepper, Mark R., “Rethinking the value of choice: A cultural perspective on intrinsic motivation”, Journal of Personality and Social Psychology 76, no.3, (1999): 349-366, https://doi.apa.org/record/1999-10261-001?doi=1
[13] Ploy Suebvises, “Social capital, citizen participation in public administration, and public sector performance in Thailand”, World Development, September 1, 2018, https://www.sciencedirect.com/science/article/abs/pii/S0305750X18301554
[14] Haryax Pathak, “India’s COVID-19 Vaccination Campaign: A marathon, Not a Sprint,” ORF Special Report No. 143, June 2021, Observer Research Foundation. https://www.orfonline.org/research/indias-covid-19-vaccination-campaign/
[15] Some examples:
[16] Hari Narayan, “India, a land of many tongues,” The Hindu, August 7, 2021, https://www.thehindu.com/thread/arts-culture-society/india-a-land-of-many-tongues/article19445187.ece
[17] Sohini Ghosh, “Vaccine coverage District officials in Gujarat cite ‘differences’ in estimated target population,” Indian Express, October 22, 2021, https://indianexpress.com/article/cities/ahmedabad/vaccine-coverage-district-officials-in-gujarat-cite-differences-in-estimated-target-population-7584073/
[18] Ravi Mittal, Surbhi Jain, Christopher G. Myers, Tinglong Dai, and Amit Jain, “A 100% COVID Vaccination Rate Is Possible – We Did It,” Medpage Today, October 22, 2021, https://www.medpagetoday.com/opinion/second-opinions/95203
[19]Nisreen Naaz, “Chhattisgarh: Durgapur becomes first village in Raigarh district to achieve 100% vaccination of adults,” Times of India, June 22, 2021, https://timesofindia.indiatimes.com/city/raipur/chhattisgarh-durgapur-becomes-first-village-in-raigarh-district-to-achieve-100-vaccination-of-adults/articleshow/83744518.cms
[20] Saul Kaplan, “If All of Work Were Gamified”, Harvard Business Review, May 23, 2011, https://hbr.org/2011/05/if-all-of-work-were-gamified
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Dr Ravi Mittal is an Indian Administrative Services (IAS) officer currently posted as the District Collector of the District Jashpur Chhattisgarh. He has an academic ...
Read More +
Oommen C. Kurian is Senior Fellow and Head of Health Initiative at ORF. He studies Indias health sector reforms within the broad context of the ...
Read More +