
-
CENTRES
Progammes & Centres
Location
India's upcoming presidency could be an opportunity to make global health governance more democratic and evidence-based.

In recent years, pandemics and epidemics are becoming more prevalent all over the world. The World Health Organization Director General (WHO DG) convenes the IHR Emergency Committee (EC) to determine whether an outbreak can be declared a Public Health Emergency of International Concern (PHEIC). This committee advises emergency, interim recommendations to the WHO DG. There have been seven PHEIC announcements, including monkeypox, since the adaptation of the International Health Regulations (IHR) in 2005. However, recent experience has highlighted IHR's shortcomings in designating a PHEIC whenever necessary. For instance, with the widespread proliferation of the Ebola virus in 2014, it took four months for the WHO to declare a PHEIC.
Many countries, including India, have suggested that reforms within WHO are long overdue, and the establishment of an intergovernmental body in 2021 to negotiate a new international treaty to strengthen pandemic prevention, preparedness, and response, is seen as a major step in the evolution of the global system. In the past, the declaration of PHEICs has been fraught with controversies, and the WHO has often been blamed for both acting hastily and late by different stakeholders. The IHR failed to enable WHO's rapid declaration of a PHEIC during COVID-19, delaying a proper pandemic response. With insufficient reporting and expert disagreement, the WHO DG convened the EC three times in late January 2020 to advise on the declaration of a PHEIC, as the committee stated that it was “too early” and that there were “a limited number of cases abroad”. This emphasises the necessity for a system that rebuilds current normative authority within a redesigned architecture that allows communities significant influence over the global health environment.
With insufficient reporting and expert disagreement, the WHO DG convened the EC three times in late January 2020 to advise on the declaration of a PHEIC, as the committee stated that it was “too early” and that there were “a limited number of cases abroad”.
During the 150th session of the Executive Board (EB), convened from 24-29 January 2022, the WHO DG emphasised five priority areas that needed global attention to prepare and respond to future pandemics. Five priorities are:
(i) To support countries to make an urgent paradigm shift towards promoting health and well-being and preventing disease by addressing its root causes,
(ii) To support a radical reorientation of health systems towards primary healthcare, as the foundation of universal health coverage,
(iii) To urgently strengthen the systems and tools for epidemic and pandemic preparedness and response,
(iv) To harness the power of science, research innovation, data and digital technologies as critical enablers of the other priorities, and,
(v) To urgently strengthen WHO.
However, during monkeypox, COVID-19, and the previous PHEICs, there was a reported lack of coordination amongst state members and WHO IHR recommendations. One factor was the lack of involvement or adequate representation of states from all regions in decision-making. In this context, to ensure coordination among EC, DG, EB, and World Health Assembly (WHA) members, the Government of Austria proposed Standing Committee on Pandemic and Emergency Preparedness and Response (SCPPR). This paper argues that a system like SCPPR is relevant during a pandemic. SCPPR-like systems are also viable even in an ongoing PHEIC monkeypox epidemic.
During the second meeting, the WHO DG vetoed his authority to declare monkeypox a PHEIC, which was supported by few and opposed by other EC members, demonstrating a lack of coherence between the WHO DG and the EC.
The WHO DG organised two meetings in response to the decision to classify monkeypox as a PHEIC. During the first meeting, no consensus was reached. However, during the second meeting, the WHO DG vetoed his authority to declare monkeypox a PHEIC, which was supported by few and opposed by other EC members, demonstrating a lack of coherence between the WHO DG and the EC. An SCPPR-like system could be a good argument for involving states in decision-making while ensuring coordination and transparency. In the following paragraphs, we argue how different member states regard SCPPR, the similarities and differences in perspectives, and how SCPPR can contribute to evidence-informed decision-making.
The scope of SCPPR would be to provide guidance concerning proposals on pandemics and emergency preparedness and response. It would also assist the DG in considering temporary recommendations in the event of PHEIC and also assist EB and WHA on policy issues upon the declaration of PHEIC. SCPPR has the potential to narrow the gap between WHO’s scientific advice given by the secretariat and expert committees (evidence-based policymaking) and policies in action in member states (evidence-informed policymaking) which would also strengthen the role of member states in guiding the DG. During the pandemic, SCPPR can bridge the gap between an emergency committee of IHR and EB. In the current system, there is no direct linkage between EC and EB members. However, member states differed in opinions related to the scope and purpose of SCPPR.
The Government of Austria acknowledged the issues the member states raised and reiterated that further discussion and revision on the ToR would be done to ensure clarity.
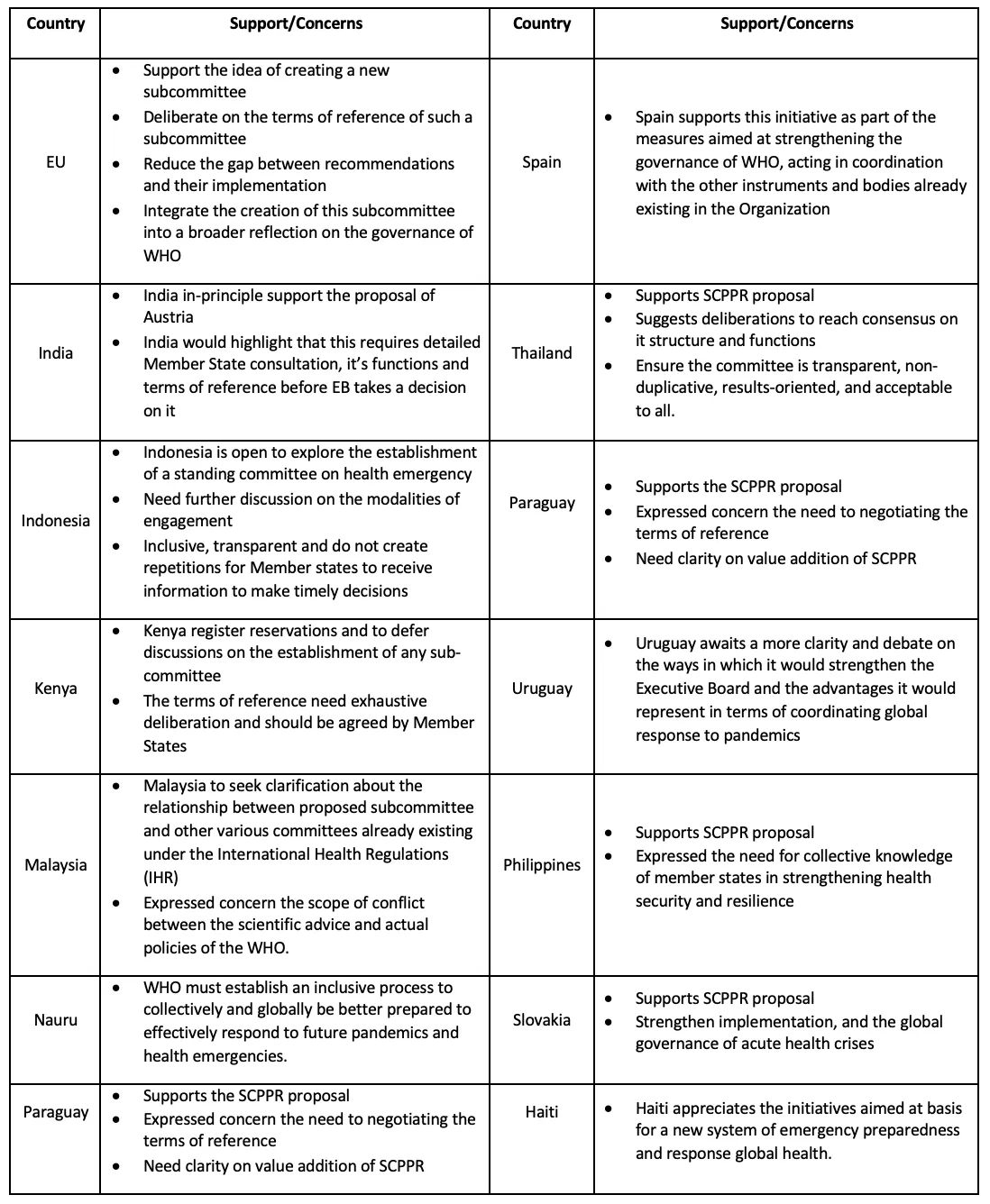
The majority of member states endorsed the proposal by the Austrian government to establish SCPPR during the EB session with some reservations. For example, some member states have expressed concerns about the lack of clarity of structure, functions, and terms of reference (ToR); Thailand stressed the need to be transparent, non-duplicative, results-oriented, and acceptable to all. Spain and Haiti had no specific reservations as they welcomed the establishment of SCPPR. The Government of Austria acknowledged the issues the member states raised and reiterated that further discussion and revision on the ToR would be done to ensure clarity.
In addition, although supportive of the proposal, Malaysia expressed concern regarding the possibility of conflict between the proposed subcommittee and existing committees under the IHR. Similarly, Ghana raised concerns over bypassing decisions made by EB members (Table 1).
Table 1: The member states’ statement on SCPPR
In line with Shannon and Weaver's model of communication, the authors advocate the Evidence- Informed Pandemic Support System (EIPSS) framework that can leverage and support strengthening communication between the states and communication among WHO-DG, EC, WHA, and EB members (Figure 1). It is a system of feedback loops that indicates progress direction and calls immediate attention to matters requiring a course correction. The member states representing the standing committee may consult with the existing EB members for clarification and recommendations (in dotted line), which will increase transparency and facilitate decision-making. We believe the framework will bring clarity and efficiency by encapsulating the interlinks between EC of IHR, DG of WHO, EB, and WHA. The EIPSS framework will facilitate effective communication among all the stakeholders, from evidence-based policymaking to evidence-informed policy enactment and outcomes. For instance, EIPSS, represented by member states, can support the EC of IHR, and DG of WHO in the ongoing work concerning policy proposals on pandemics and emergency preparedness and response plans.
Figure 1: Evidence-Informed Pandemic Support System (EIPSS) framework
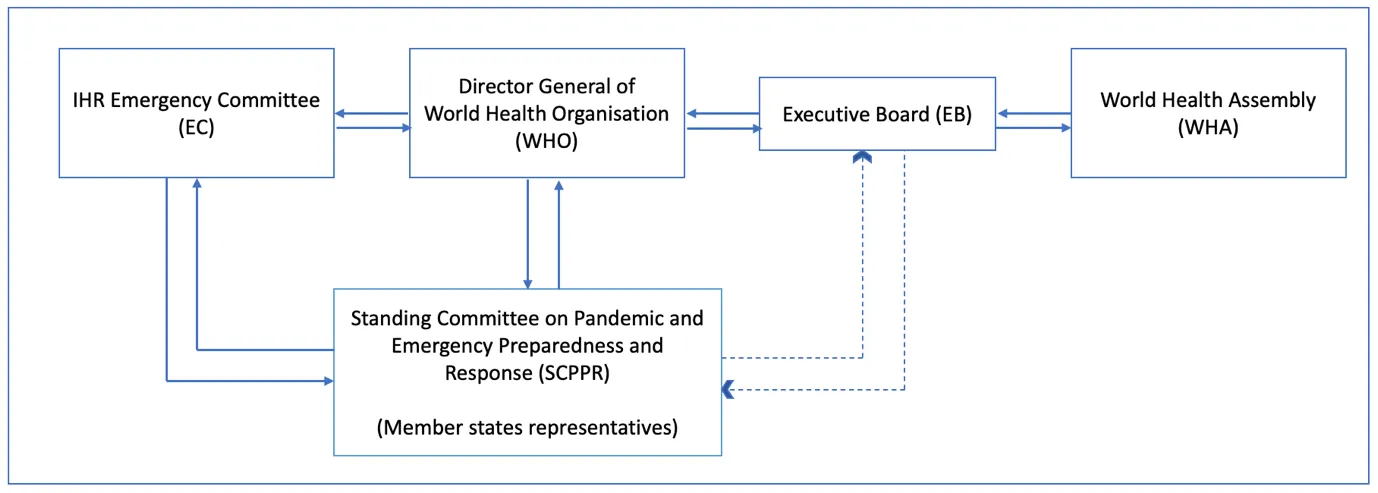
SCPPR can build trust and rapport during crises by supporting IHR, the DG, and EB members. In the EIPSS framework, SCPPR will follow the line of communication as per the norms of WHA, and there is no bypassing of EB members. SCPPR is mainly a support system for effective coordination and communication with limited decision-making roles. Its role is to facilitate the sub-committee to bring consensus among EB members and WHA in line with IHR temporary recommendations.
Over the recent past, G20 Joint Finance and Health Task Force (JFHTF) has emerged as a major global platform for discussing efforts to prevent, detect, and respond to health emergencies. The upcoming G20 presidency of India could be an opportunity to make global health governance more democratic as well as evidence-informed. Multilateral institutions need to adapt reforms for future initiatives for good governance, as the burden to translate shared scientific insight into evidence-informed global policy standards rests on these institutions. The only way for governments to better protect their populations from global health threats such as the COVID-19 pandemic is to construct a more effective communication network. In conclusion, SCPPR is one example of demonstrating the need for a committee to represent member states rather than solely subject experts during decision-making. To foster cooperation and collaboration, we require evidence-informed decision-making to assist the EC during PHEIC decision-making. Having member states represented will aid in making evidence-informed decisions.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Miss. Viola Savy Dsouza is a PhD Scholar at Department of Health Policy Prasanna School of Public Health. She holds a Master of Science degree ...
Read More +
Dr. Sanjay M Pattanshetty is Head of theDepartment of Global Health Governance Prasanna School of Public Health Manipal Academy of Higher Education (MAHE) Manipal Karnataka ...
Read More +
Prof. Dr.Helmut Brand is the founding director of Prasanna School of Public Health Manipal Academy of Higher Education (MAHE) Manipal Karnataka India. He is alsoJean ...
Read More +
Oommen C. Kurian is Senior Fellow and Head of the Health Initiative at the Inclusive Growth and SDGs Programme, Observer Research Foundation. Trained in economics and ...
Read More +


