Health Systems Resilience Index: A Sub-National Analysis of India’s COVID-19 Response
Foreword
Dr Samir Saran
There is no better time than now to invest in health systems. More than two years since the outbreak of COVID-19, societies and economies across the globe are still straining from the impacts of the pandemic. Even the big economies that were presumed to have well-equipped healthcare systems were rendered helpless by a virus that was determined to reach every territory across the globe. We all re-learnt a lesson we had archived in the recesses of our minds: that health security and protecting life must continue to be not only a central state policy, but our societal obsession, too. Equally crucial, we were taught that to manage a health crisis of the magnitude of COVID-19, we must nurture effective and objective emergency communication, adaptive socio-economic behaviour, and the ability to mobilise and deploy resources. For all of this, political and social leadership remains an imperative.
In India, a healthcare delivery system that has historically suffered from ad-hoc regulation, poor monitoring, and modest budgetary allocations, needed to be streamlined rapidly to fight the pandemic. Some states and union territories (UTs) succeeded more than others. For those who did, the key was aligning their health systems with the needs of the population. Today, as the world sees a likely future of recurring infections, state leaders will need to prioritise the building of knowledge systems and investment in human capital and critical infrastructure, and to put into place robust evaluative mechanisms. This will need an across-the-board consensus for action.
This ORF report presents a sub-national analysis of India’s health system, which takes into account both the tangible and intangible assets at the state level against the backdrop of the pandemic. This pioneering Health Systems Resilience Index is composed of five sub-indices that use 33 indicators covering quantifiable aspects of the resources and governance mechanisms that were available to, and were wielded by India’s states and UTs. Utilising publicly available data from various government sources, this report gives a clear view of how the states and UTs fared during the 2020 and 2021 waves of COVID-19; while the report ranks states and UTs on the basis of their performance, the aim is to offer a data-driven examination of the gaps in the system that can be addressed to mitigate future crises. This is the time to learn, and more importantly, the time to learn from each other across state boundaries even as we invest in global knowledge and response networks.
As unprecedented as the COVID-19 crisis has been, it will not be the last. We are required to strengthen our health systems and make them harmonious, equitable, and sustainable. It would do us well to start doing this now.
Let me congratulate the lead authors and the ORF research team that have worked on this report. I am sure it will offer valuable inputs to policymakers and to others studying the pandemic.
Executive Summary
1. Introduction
India’s COVID-19 battle will be told and retold in the coming years, inspiring both praise for what the country has achieved, and critique for its shortfalls. As India’s story continues to unfold, two strands will mould the various assessments. First is India’s aggregate performance as a developing economy: It marshalled its meagre resources to respond to the exponential threat of the virus, and was determined, too, to be part of global solutions to this scourge, such as the manufacture and supply of life-saving vaccines. The second, and perhaps even more important story is on ground-zero: In its cities and villages, India’s success or failure would be a factor of the leadership and stewardship of Prime Minister Narendra Modi and his team in responding to the crisis, and the commitment of the chief ministers and state functionaries to beef up their health systems and save lives.
Whichever way the India story is told, there are certain truths that cannot be hidden: We need to invest more in our health systems, and acknowledge the stellar role of our frontline workers and formal and informal health sector personnel, as well as India’s prowess in certain segments of the medical and health industry.
In this context, it becomes interesting to see how in the country’s federal structure (where health is a State subject), the sub-national units—i.e., states and union territories (UTs)—have performed. The present work,Health Systems Resilience Index: A Sub-National Analysis of India’s COVID-19 Response,provides answers to that question. It builds on an earlier report published by the Observer Research Foundation in May 2020. That report,State of the States: Two Months of the Pandemic, evaluated India’s initial response to the pandemic shortly after the crisis was officially named by the World Health Organization (WHO). Two years since then, this report attempts a more ambitious goal: to devise a unique Resilience Index for the health systems of India’s states and UTs.
2. About the Report
The report has two distinct components presenting the state of health systems on the basis of various parameters and reports on the resilience of such systems. It begins with a presentation of individual states and UTs’ health profiles, in the context of the pandemic, using publicly available data. All data variables considered for this study were collated from Government of India sources and are available in the public domain. Not a single data has been sourced from a non-governmental origin. On the basis of government data, the report presents a new composite index—one that encapsulates a comprehensive evaluation of the level of resilience of each state and UT that considers the COVID-19 pandemic as a “stress test” for health systems.
3. The Health Systems Resilience Index (HSRI)
3.1 Motivation and need for a composite index for health systems resilience
The prolonged COVID-19 pandemic has served as a “stress test” for India’s health systems. Did those systems pass the stress test, or did they fail? More importantly, have those systems been strengthened since, in order for them to become more resilient in the event of subsequent waves of COVID-19 or another health crisis of similar magnitude? These are the key questions that needed to be answered as current health policy literature has not attempted to do so.
It needs to be kept in mind that Health is a State Subject. The Union Government’s role is largely prescriptive by way of policy and drug control. However, a disaster of the scale such as that of the pandemic required the Union Government to invoke the Disaster Management Act 2005 and the Epidemic Diseases Act 2020 to intervene.
Yet, that does not take away the responsibilities of the sub-national entities, their initial infrastructure and endowments, and their responses to the outbreak of COVID-19, especially during the disastrous first and second waves.
3.2 Methodology and Data Sources
The index was developed using 33 component indicators, classified into five broad parameters or sub-indices, namely: general health profile; medical infrastructure; technology infrastructure; institutional support; and COVID-19-related health outcomes (see Table ES1). Therefore, the composite index is a combination of initial conditions that are reflective of the health preparedness of a sub-national unit, the response mechanism to the pandemic, and the final outcomes. In another sense, the index is a combination of static variables (those under General Health Profile, Medical Infrastructure, Technology Infrastructure, and the two revenue expenditure variables under institutional support, and the vaccine doses, tests, deaths, peak daily case load under COVID-19 related health outcomes) and dynamic variables (the two related to revenue change under institutional support, and the time taken between the highest peak of daily cases to its 20 percent, time taken between peak positivity rate to fall below 5 percent, days taken to reach benchmark vaccination coverage of 18+ population, and weeks taken to reach benchmark vaccination coverage of 60+ population under COVID-19-related Health Outcomes.)
Table ES1: Sub-indices, Indicators, and their Data sources
All the indicators use government data as their primary sources. Even theCOVID19 Bharat Dashboardcollates data from governmental sources. All the indicators were normalised and scale biases were removed. The weights were assigned at two stages: at the level of the individual parameters, Principal Component Analysis (PCA) was conducted with 33 component indicators; in the second stage, weights were dictated by informed arbitrariness. The combination helped in simultaneously capturing the variations in capacities and performances of health systems across the various sub-national entities (See Annexure II for further details on data sources and the methodology).
3.3 Key Findings
The detailed findings on the relative performances of the states and UTs are available in section 3 of this volume. Other details on the methodology and results on indicators are provided in Annexures 2 and 3. Some of the key findings are as follows:
In terms of the composite scores of HSRI, Goa ranks at the top of all small states, Himachal Pradesh above all large states, and Lakshadweep among the UTs.
There is a significant difference between the average level of resilience in health systems among the states and the UTs, with the UTs performing better (and the difference is found to be statistically significant at 1% level).
States and UTs with higher per-capita income levels are significantly more resilient to combat a potential new wave of the pandemic or any other health crisis of similar magnitude, than the poorer regions.
Meghalaya has done exceedingly well in the domain of institutional support to the health sector. Himachal Pradesh and Sikkim also did relatively well among the remaining states, followed by other small states like Tripura, Goa, and Mizoram. Jammu & Kashmir leads among the UTs.
Himachal Pradesh, among the large states, and small states like Goa and Tripura have done better than other states in the management of COVID-19-related Health Outcomes. Among UTs, Lakshadweep and Andaman and Nicobar Islands show noteworthy results, even outperforming all states.
Tamil Nadu and Chhattisgarh (among the larger states) and Goa (among the small states) have the best records in their General Health Profile; among the UTs, Dadra & Nagar Haveli and Daman & Diu are the leaders. A notable aspect is that a high score on General Health Profile has not ensured a high score on COVID-19-related health outcomes for the larger states; rather the pattern is quite the opposite. In Medical Infrastructure, smaller states such as Arunachal Pradesh, Sikkim, and Mizoram have the best population-level services as do larger states like Kerala and Maharashtra. Among UTs, Lakshadweep is most equipped.
Goa, among the small states and Tamil Nadu and Kerala, among the large states fulfill the most number of criteria for Technology Infrastructure. Delhi leads among the UTs.
Table ES2 shows the HSRI scores and rankings.
Table ES 2: Health Systems Resilience Index Scores and Ranking
4. Summing-up
More than two years since the first cases of COVID-19 infections were reported in India, the country is now in the midst of recurring infections. Armed with scientific knowledge—not only of the virus that causes COVID-19 but of life-saving vaccines as well—India must, more crucially now than ever, fill the yawning gaps in the country’s health systems. This task will be possible through better data infrastructures to drive policy, and an aggressive push towards Universal Health Coverage. Given that India opted for a phased vaccination process beginning with the most vulnerable groups of the population, the figures of 73.5 percent with a single dose and 69 percent fully vaccinated at the time of finalising this report are indeed remarkable. The following months will see the step-by-step deployment of booster doses for India’s remaining population.
The imperative is a collective and targeted effort to scale the immunisation initiative while adhering to COVID-19-appropriate behaviour as a population. India must learn from the past three waves and ramp up investments in health and develop sound strategies for expected future waves. Scientific endeavours and behavioural changes are also essential to minimising the impacts of another sudden increase in infections, and even deaths. The past two years of battling the pandemic forced our health systems to a redesign. Today, as new emergencies emerge in a matter of days, key will be the readiness of systems to respond and mobilise resources efficiently.
This report aims to help light the way for India. Utilising a Resilience Index for States and UTs, this study offers insights into the state of the country’s health systems at a disaggregated sub-national level, and the parameters that need to be addressed in the short term. This assessment should pave the path for more researchers and scholars to conduct further research in the domain of comparative spatial assessments, and probe the resilience of health systems to shocks. A similar exercise can be undertaken at the global, local, and micro-levels, to determine the effectiveness of existing healthcare ecosystems in responding to various crises.
This report could be useful for decision-makers as it creates a framework for understanding what works and what does not, and therefore guide necessary course-correction along the way. The public, too, would find this report useful as they seek to engage with India’s democratic architecture.
Introduction
In January 2020, as the world heard the first reports of the novel coronavirus, the medical community had little data with which to formulate responses that could alter the rapid trajectory of what was then an epidemic. Shortly thereafter, in March, the World Health Organization (WHO) declared the outbreak of SARS-CoV-2 a pandemic, and countries immediately implemented lockdowns and restrictions on movement. In India, the first two months of the pandemic saw over 80,000 cases and 2,700 deaths despite a country-wide lockdown from late March.[1]It was at the time that ORF released its report,State of the States: Two Months of the Pandemic,which analysed, with the help of emerging data and anecdotal evidence, the initial impact of COVID-19 on India. The key priority then was to delay the spread of infection until health systems could be reinforced and resources ramped up to handle the outbreak.
It helped that the number of medical seats in the country had been increased in recent years—this eased the human resource constraints during the pandemic, as India roped in trainee doctors and medical students to work on the frontlines. Indeed, the last decade saw public investments being channeled to the country’s tertiary healthcare sector—in particular, in the supply of health workforce: between 2014 and 2019, there was a 47-percent increase in the number of government medical colleges, and a 33-percent rise in private medical colleges. The number of undergraduate medical seats also saw a jump of 48 percent, from 54,348 in the academic year 2014-15 to 80,312 in 2019-20. While India was expanding the number of seats in government medical colleges, it was also leveraging the private sector to fill gaps in personnel and healthcare delivery.[2]
Over the past decades, India’s health outcome indicators have shown consistent improvement, much of it being achieved despite inadequacies in both policy attention and financing. When the National Health Policy 2017 set a target of allotting 2.5 percent of GDP to government expenditure in health by 2025, most analysts were of the view that the goal was highly ambitious. The next three or so years will reveal whether India reaches that target, and if the COVID-19 pandemic will prove to be a motivation. The Union budget of 2021 announced a new centrally sponsored scheme, the PM Atma Nirbhar Swasthya Bharat Yojana with an outlay of INR 64,180 crores over six years, aimed at developing the capacities of primary, secondary, and tertiary care systems and strengthening capacities from detection to cure.[3] However, despite such schemes and the financing of the massive COVID-19 vaccination and screening efforts, the health sector outlays have remained low even during the pandemic years. Even the 2022 Union budget—which provides that the outlay for capital expenditure be enhanced by 35.4 percent from INR 5.54 lakh crore last year to INR 7.50 lakh crore, left the health sector largely untouched.[4]
Government agencies at the forefront of the COVID-19 battle have had to do with the limited resources at their disposal. In April 2020, the Ministry of Health and Family Welfare instituted a three-tier COVID-19 Treatment system to facilitate triaging and thereby maximise constrained supplies.[5]The first line of testing and detection was assigned to Fever Clinics or local health centres. Suspect or positive patients then moved through the bottom-up, three-tiered structure, from COVID-19 Care Centres to Dedicated COVID-19 Hospitals. Care Centres ensured bigger spaces for isolating both symptomatic and asymptomatic, very mild cases. Tier-2, Dedicated COVID-19 Health Centres are for mild to moderate cases, and the most severe, symptomatic cases were referred to Dedicated COVID-19 Hospitals.
While most states have followed the three-tier structure, some like Kerala have added further levels of management based on criteria such as space for isolation and need for medical monitoring. Meanwhile, a number of states have not set up Fever Clinics at all. Delhi, for instance, decided to employ its own network of Mohalla clinics for preliminary diagnosis and surveillance.
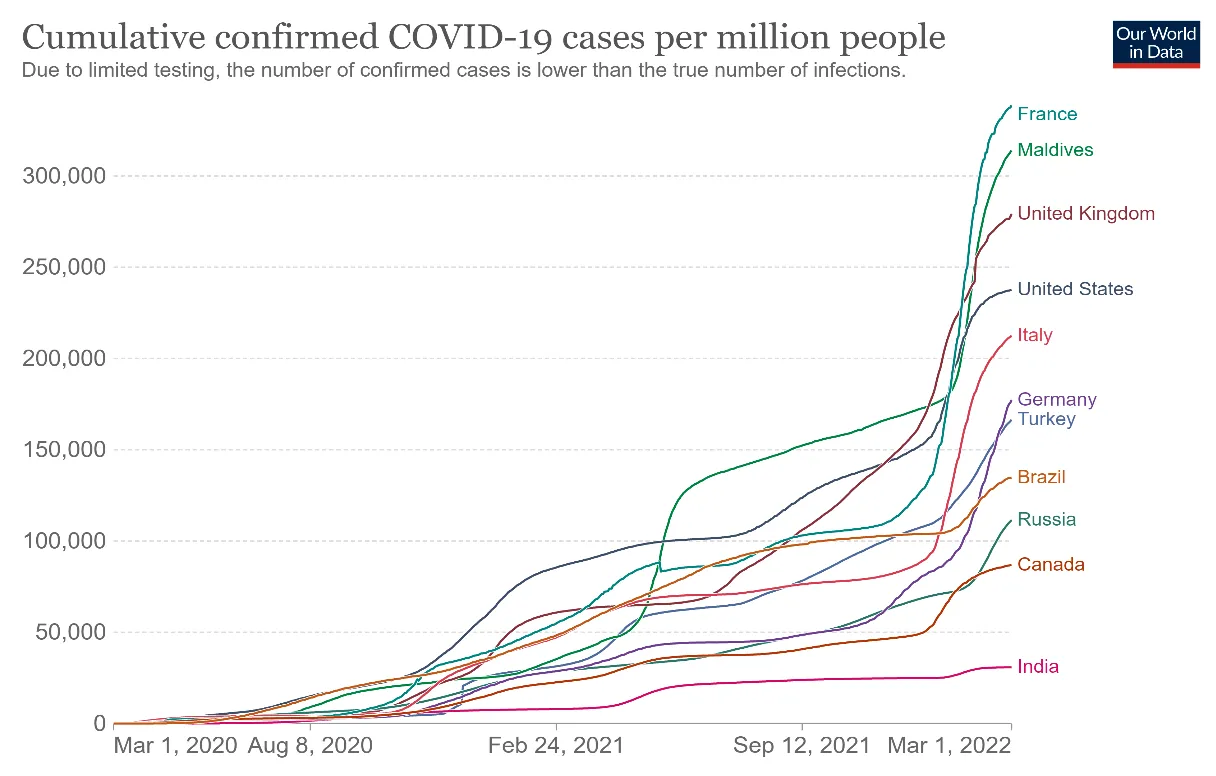
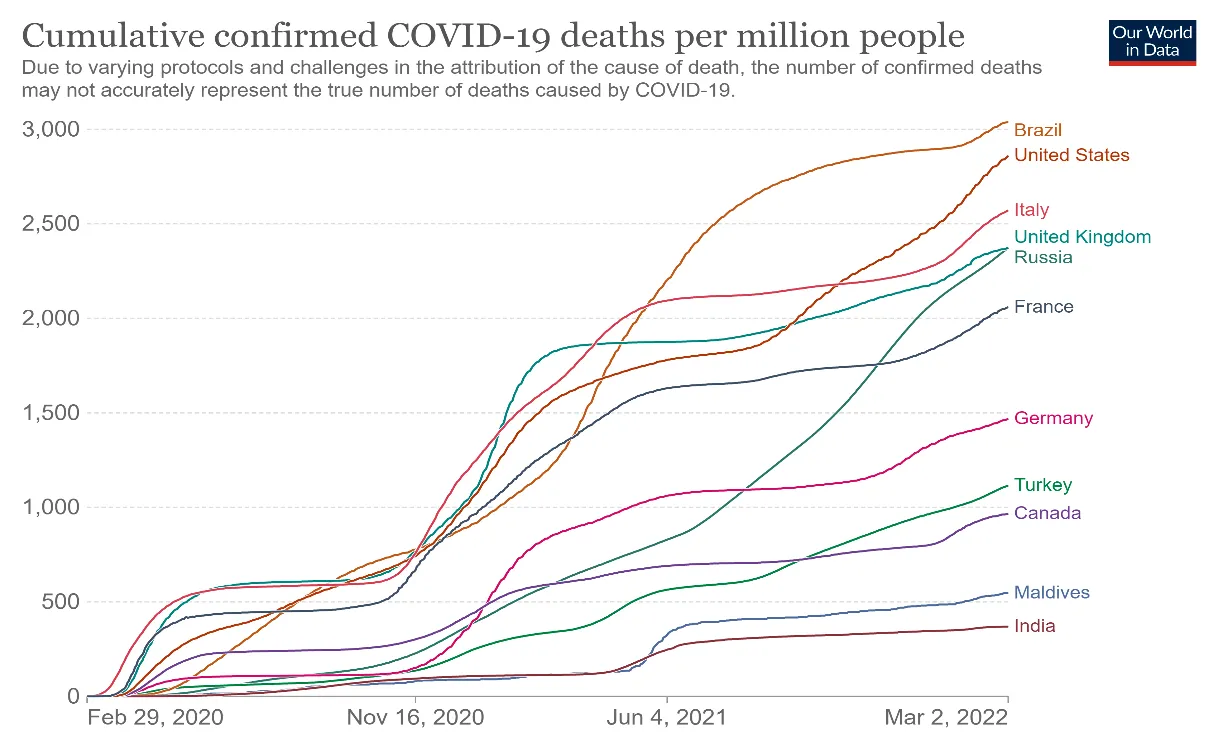
At the time of writing this report, almost 500 million COVID-19 cases have been confirmed globally. India has recorded nearly 42 million of these cases, amounting to about 31,000 cases per million people. The country officially recorded close to 370 deaths per million population. It ranks much lower in both cases and deaths when compared to advanced economies, with notably smaller countries facing a bigger burden on its population-level impact.
Figure 1: Cumulative Confirmed COVID-19 Cases per million across the World
ORF’s own research has catalogued India’s dogged efforts to manage the COVID-19 crisis.[8]India’s performance becomes even more remarkable with the massive vaccination drive that covered the largest numbers of population in the shortest period of time. Indeed, on some parameters, India has performed better than certain developed nations that claim to have far superior infrastructure and higher healthcare spending (see Figures 1 and 2, and the vaccination numbers).
India has vaccinated 73.5 percent of its population with a single dose, and 69 percent are fully vaccinated. These figures become more notable when compared to a country like the US, for example, whose size is one-fourth that of India’s but has fully vaccinated a lower 66 percent of its population. The ensuing months will witness how India fares in the step-by-step deployment of booster doses for the remaining population.
At the same time, however, the apparent success story at the macro-level is not reflective of the nation’s chequered pandemic journey: a pathway fraught with tremendous challenges at various points.
India began with a degree of success in mid-2020 because of the swift lockdowns and focused promotion of appropriate COVID-19 behaviour such as regular handwashing, the wearing of masks, and physical distancing. Eventually, restrictions were eased, and the first wave peaked in September 2020. The sharp rise in cases was attributed to poor adherence to masking and appropriate behaviour during the festive season. Cases and deaths would thereafter fall sharply, until a massive second wave in April and May 2021 ended the notion that India had been able to contain the pandemic and the crisis had met its end. The degree of transmission was so intense that the sero-positivity rate increased from 24.1 percent in January 2021 to 67.6 percent in July 2021.[9]By early May, the death rate had spiked to almost 4,000 people every day.
As steep as these numbers are, however, they are possibly still higher on the ground.[10]The under-counting could be the result of a number of reasons: sub-national discrepancies in scientific standards and definitions; delayed penetration of COVID-19-related preventive services into sub-urban and rural areas; and weak data and communication systems. Evidence suggests, for example, that socially vulnerable populations like women and the poor are often left out of surveillance simply because the health-seeking behaviour of these groups are unaccounted for in planning.[11]
After the cruel second wave, there have been efforts to calculate “excess” deaths during the pandemic. ALancetstudy estimates 4.07 million excess deaths in India compared to the official number of half a million between January 2020 and December 2021.[12]WHO’s recent estimates show a similar statistic.[13]Computations by Indian scholars, too, have suggested excess deaths to be nearly eight times the official figure.[14]Further, a model byThe Economistputs excess deaths in India between 1.9 million and 9.7 million by end-2021.[15]The range of these estimates is wide, owing to uncertainty about the quality of both data sources and assumptions.[16]The Union Government quickly denied the estimates, because all the models are based on a host of hypothetical assumptions of conditionalities, and their functional forms largely deviate from real-life conditions.
Recounting and adding backlogs are not easy tasks, given the varying degrees of institutionalisation of medical care across the country and the changing definitional guidelines for classifying deaths due to COVID-19. According to ORF’sCOVID-19 Tracker, about 86,000 deaths have been added as backlogs[17]between June 2021 and March 2022—or about 16 percent of all reported COVID-19 deaths in India today.[18]However, only 19 states and UTs ever reported backlogs in deaths. Bihar and Kerala added more than 50 percent of all their COVID-19 deaths through backlog counting and compensation appeals.[19]Other states like Karnataka, Madhya Pradesh, Maharashtra, and Tamil Nadu have also been consistently adding numbers to their logs. Media reports also point to much higher numbers ofex-gratiaclaims for compensation of COVID-19 deaths, compared to the reported numbers.[20]
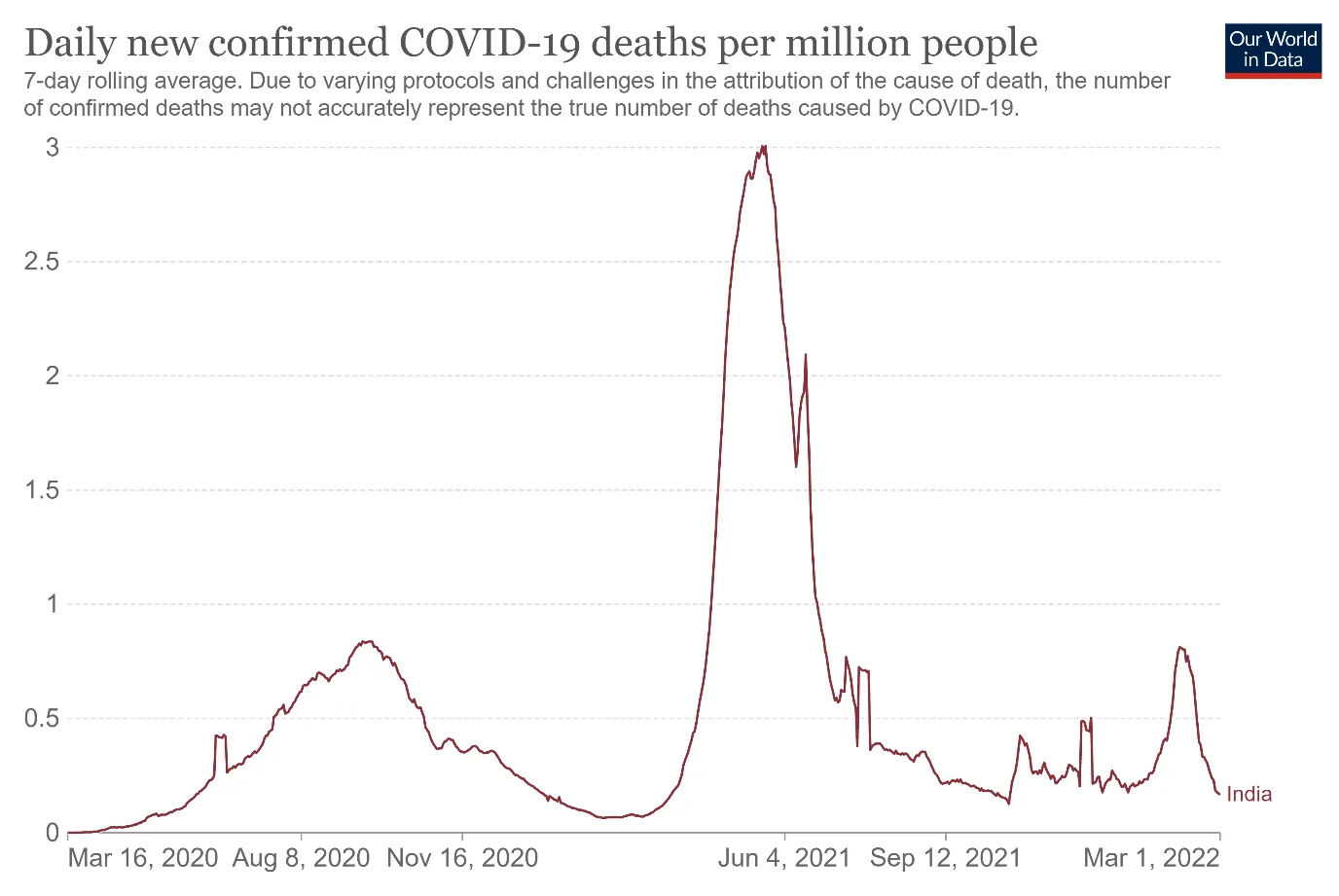
Yet, 2021 was not only about rapid transmission dynamics and mounting deaths; it was also the year that the vaccination rollout was initiated. The drive faced acute shortages shortly after being started in January 2021, but eventually picked up pace and accelerated in the latter part of the year. India is currently using four vaccines, and ten more have received emergency approvals.[21]As of 15 March 2022, more than 80 percent of the population above 45 years of age, and 75 percent of the 18-44 cohort, are fully vaccinated. The coverage for the younger group of 15- to 17-year-olds is at 46 percent. At its current levels of mass inoculation, India has come closer to community-level protection as milder infections continue to help build natural immunity against the virus. Figure 3 shows the patterns of this attuned immunity—even through the Omicron-led third wave, hospitalisation and deaths remained largely consistent and low.
Figure 3: Daily New Confirmed COVID-19 Deaths in India
This report offers a uniqueHealth Systems Resilience Indexthat measures how, and to what extent states and regions across India have adapted to the COVID-19 crisis and grew in capacities over the past year. Each state and UT is profiled in three broad areas: (a) their current health profile—which uses indicators such as demographics (as per the 2021 projections), 2020 ranking in Sustainable Development Goal 3 (Good Health and Well-being), regular vaccination coverage for under-fives, out-of-pocket health expenditure, and causes of mortality; (b) COVID-19 preparedness and response (which offers a population-level description of the states’ medical infrastructure, technological response, and government investments); and (c) COVID-19 cases, deaths, tests, and vaccination.
While the initial research for this study was conducted in early 2021, the last leg of the data collection was ended in November-December 2021. The development of the index, and the writing and production of this report was all done in early 2022, as the highly transmissible Omicron wave of COVID-19 was receding in India, even as the country continued to reel from its impacts. Unlike the Delta-led second wave, which was gradual in its ebbs and flows and yet far more fatal, the third wave was rapid to rise and equally quick to fall, with considerably lower incidence of hospitalisation and less fatalities, too.[23]
The daily reported cases have come under 5,000 at the time of writing this report, and life is slowing getting back to normal as children have gone back to school and even recreational facilities are operating at full capacity. The high level of vaccine coverage and infection-induced natural immunity has kept fatalities low during the third wave led by the Omicron variant and its sub-lineages. Despite the rapid pace of vaccination, subsequent waves of the virus may still recur in the coming months, given the very nature of a pandemic—i.e., prolonged, with repeated waves of infections. It is vital to reassess the situation and re-strategise the country’s preparedness.
India has historically suffered from a scarcity of timely and quality data that could inform crucial decisions on healthcare, though the situation has started improving over the last decade. Optimally utilising available data sources, this report offers a data-driven perspective of the performance of India’s 28 states and eight UTs during the first two years of the COVID-19 pandemic. It proceeds from the assumption that because Health is a State subject, policies and strategies are planned and executed according to each State’s priorities. State capacities and instruments mediate the health sector’s financing and governance capabilities, and programme implementation may vary significantly across different states.
In practice, the Union Government has so far played a largely prescriptive role through policy and drug control. But COVID-19 was an exogenous shock that disrupted the fundamentals of the socio-economic architecture of the global economy, as well as those of individual countries, including India’s. The sheer scale of the pandemic required the Union Government to invoke the Disaster Management Act 2005 and the Epidemic Diseases Act 2020. That does not take away the responsibilities of the sub-national entities, their initial infrastructure and endowments, and their responses to the outbreak, especially during the disastrous first and second waves.
Meanwhile, there is a view that both the states and the Centre should have legislative powers over healthcare, and in 2019, the High-Level Group on Health constituted under the Fifteenth Finance Commission made precisely this recommendation—i.e., shifting healthcare under “Concurrent Subjects”.[24]While the implementation of such a recommendation is pending, any assessment of crisis response is best conducted at the sub-national level. The question remains as to how, in India, “cooperative federalism” can minimise “conflictual federalism” and bring the pandemic under control.[25]A comparative analysis of the prospects of India’s states and UTs confronting the challenges of a likely next COVID-19 wave—or another health crisis of similar magnitude—can guide policymakers towards an efficient roadmap.
Notes on Structure, Methodology, and Sources
This report is divided into four main sections: Following the Introduction, Section 2 provides an overview of individual states and UTs; Section 3 introduces the Health Systems Resilience Index, and ranks the states and UTs on a comparative scale of quantifiable indicators within specific themes to assess their respective health systems. Section 4 concludes the report.
Section 2 offers the reader a comprehensive view of the performance of each state. The elements in the state profiles include other parameters that were not available yet at the time of publication of ORF’s firstState of the Statesreport. These include the numbers of COVID-19 dedicated three-tier health facilities and beds, testing laboratories, and sample collection centres; the technological innovations and investments; as well as parameters on data reporting and granularity.
Each state and UT profile is divided into three sections: general health; COVID-19 preparedness; and government response. The report provides graphical representations of COVID-19 trends and preventive measure of cases, deaths, tests and vaccinations over a span of 20 months. The COVID-19 statistics were culled from a credible, volunteer-driven data platform,COVID19india(later continued by COVID19bharat collective), which collates numbers from information bulletins officially released by the respective state governments or their health ministries.
The General Health Profile of the state or UT includes indicators such as age-wise demographics, population density, regular immunisation coverage, out-of-pocket expenditure in health, insurance coverage, top causes of mortality, death rates – both general and related to COVID-19, and per capita revenue expenditure of the state for medical and public health and family welfare. To provide already established scales of evaluation for states’ performances, the report also uses the Bare Necessities Index (Economic Survey 2020, Ministry of Finance) and the SDG 3 India Index for Good Health and Well-being (2020). The scales cover a wide range of social determinants of health.
Immunisation programmes and health spending are discussed as well, using data from the National Family Health Survey 5 (2019-20). Per capita out-of-pocket health expenditure data has been sourced from NITI Aayog’s SDG Index 2020.
It is well-established that comorbidities are significant catalysts of mortality and morbidity in COVID-19 infections. While there is a range of medical conditions to study in this spectrum, the researchers have chosen Diabetes and Kidney Diseases, Neoplasms (Cancers), Respiratory Infections and TB, and Cardiovascular Diseases—this is because these diseases cover a gamut of known leading non-communicable diseases for which proper treatment is crucial. The data on the prevalence of such NCDs and the death rates have been taken from a pre-COVID-19 period (2019)—to reflect the pre-existing risk factors in the respective states. The data is sourced from theGlobal Burden of Disease: India Compare Study (2019)by Institute for Health Metrics and Evaluation (IHME) and Public Health Foundation of India (PHFI). Moreover, these comorbidities are more predominant among certain age groups who are thereby more vulnerable to a contagion. Therefore, an age-wise composition of the state’s population has been computed in accordance with the government’s vaccine policies of under-18 years, 18-44 years, 45-60 years, and 60+ years age groups. The distribution has been computed by the research team using estimates from the Census 2021 projection of population, a detailed process of which is discussed in a latter section of this report.
The section on Preparedness and Response focuses on Medical and Technological efforts to leverage better COVID-19 management. It covers human resources, the physical infrastructure of hospitals, health centres, care centres, laboratories, and vaccination sites, as well as the technological groundwork and initiatives unique to each state and UT. The SDG Index provides the number of doctors, midwives, and nurses, while the National Health Profile (2020) provides the number of registered pharmacists within the state or UT.
The technological response was chosen for this section because the pandemic necessitated a push towards adopting new technologies. The idea was to explore whether the innovative solutions being brought to these areas truly benefit these populations. There has been a historical mismatch between the digital skills across gender, class, caste, and rural-urban divide in the country. At the same time, data is scanty on how these new technologies have been adapted and if the target populations are able to access them.
The crisis also pushed governments to creatively leverage existing technologies like IVRS, Geo-tagging, Geo-fencing, and GPS, while advancing towards more cutting-edge innovations in Machine Learning and Artificial Intelligence to ease the burden on their human resources. These new technologies, in the past two years, were adapted and implemented aggressively for better surveillance and monitoring, contact-tracing, information dissemination, diagnostics, and remote assistance. Since these are essential platforms for multi-sectoral interactions with the health system for better management, this section puts into perspective the overall numbers of mobile-phone and internet users in the state or UT. This can help assess current connectivity capacities and the reach of state-led technology initiatives in the grassroots.
All these parameters need government support to take effect. Therefore, ‘Institutional Support’ focuses on budgetary allocations and dedicated COVID-19 management and related financing from the 2021-22 Budgets. It gives a picture of the state’s pandemic governance priorities and post-pandemic plans. For individual state profiles, the budget highlights have been collated from Budget documents and mainstream media reports.
The third section of this report introduces the Health Systems Resilience Index. The resilience index is a composite measure comprising five sub-indices based on the elements discussed in Section 1. The context for the development of the index, along with its structure and methodology, is discussed in detail later in the report; more information is provided in the Annexure.
Much of the data is from the period between the second and third waves from August and November 2021. By then, the health facilities were less overwhelmed, and temporary setups were reduced, compared to April-May 2021 at the peak of the second wave. The state-wise graphical representations of COVID-19 statistics—Cases, Deaths, Tests, and Vaccinations—range from May 2020 to December 2021.
ORF exerted its best efforts to source information only from verified government sources. All data variables considered for this study have Government of India sources as their fundamental origin and are available in the public domain. Not a single data has been sourced from a non-governmental origin. On the basis of such data, the report presents a new composite index—one that encapsulates a comprehensive evaluation of the level of resilience of each state and UT that considers the COVID-19 pandemic as a “stress test” for health systems. A detailed list of references and their limitations is given in Annexure I. The report closes with a comparative analysis involving the states and the UTs, based on their average levels of preparedness and across different levels of per-capita incomes.
Rakesh Sood, Kriti Kapur and Oommen C Kurian, “India’s Vaccine Rollout: A Reality Check,” ORF Special Report No. 139, May 2021, Observer Research Foundation.
Sayli Udas-Mankikar et al., Turning the Tide: Is Mumbai Ready for the Next Wave?, July 2021, Observer Research Foundation.
Malancha Chakrabarty and Shoba Suri, “Winning the COVID-19 Battle in Rural India: A Blueprint for Action,” ORF Special Report No. 146, June 2021, Observer Research Foundation.
Sunaina Kumar, Shoba Suri, and Oommen C Kurian, “Preparing for the Next Covid-19 Wave: Lessons for Delhi,” ORF Special Report No. 164, October 2021, Observer Research Foundation.
Oommen C Kurian and Shoba Suri, “Covid-19 Global Vaccination Drive: The Goal of Equity in an Unequal World,” ORF Special Report No. 187, May 2022, Observer Research Foundation.
Ravi Mittal and Oommen C Kurian, “Bringing the Covid-19 Vaccine to Every Hamlet: The Story of Raigarh,” ORF Special Report No. 192, June 2022, Observer Research Foundation.
[9]Ministry of Health and Family Welfare, “COVID-19 Sero-Survey”, Lok Sabha UnStarred Question no. 904 (answered on 23rdJuly, 2021).
[25]Cooperative federalism refers to a harmonious and coordinated relationship between the centre and the state governments, in order to work on a variety of public policy programmes.
Conflictual federalism is characterised by a situation of centre-state and/or state-state clashes because of political, social, economic and other reasons, impeding the implementation of various welfare programmes and policies.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Mona is a Junior Fellow with the Health Initiative at Observer Research Foundation’s Delhi office. Her research expertise and interests lie broadly at the intersection ...
Debosmita Sarkar is a Junior Fellow with the SDGs and Inclusive Growth programme at the Centre for New Economic Diplomacy at Observer Research Foundation, India. ...
Soumya Bhowmick is an Associate Fellow at the Centre for New Economic Diplomacy at the Observer Research Foundation. His research focuses on sustainable development and ...
Renita DSouza is a PhD in Economics and was a Fellow at Observer Research Foundation Mumbai under the Inclusive Growth and SDGs programme. Her research ...
Dr. Nilanjan Ghosh is a Director at the Observer Research Foundation (ORF), India. In that capacity, he heads two centres at the Foundation, namely, the ...

 PDF Download
PDF Download