What Ails Health Systems in Africa? An Economic Perspective
There is hardly any doubt that failing health systems result in poor health outcomes and hamper progress towards the attainment of the Sustainable Development Goals (SDGs) and Universal Health Coverage (UHC). In Africa, health systems are hobbled by leadership and governance challenges, extreme shortages of health workers, corruption in procurement systems for medical products and technologies, poor information systems, and health financing constraints. This brief discusses ways in which decision-makers can hurdle these challenges.
Attribution:
Daniel Mwai & Theresa Ndavi, “What Ails Health Systems in Africa? An Economic Perspective,” ORF Issue Brief No. 431, December 2020, Observer Research Foundation.
Introduction
Most African countries gained independence between the 1950s and 1960s. In order to build their economies, import substitution policies were encouraged as a conduit for economic growth and industrialisation. Advocates of import substitution argued that developing countries should promote domestic industries and reduce their dependence on foreign trade.[1]However, this view would soon lose favour as restrictive trade policies resulted in economic costs. Moreover, it was noted that the benefits of a more outward-looking, export-oriented approach to trade and development far outweighed the costs of import substitution. Between the early 19thto mid-20thcentury, due to the consequences of slavery and colonisation, Africa was left behind when other countries industrialised their economies. When African countries finally moved into the international trade space, a majority of the commodities from the continent were raw materials traded for finished products. This meant that African countries gained little from trading with other countries, and because of slow industrialisation, these countries had to continue to import finished products at a higher price. This was due to lack of skills, capital, infrastructural support, technology and markets—which encouraged inefficiencies in the industries, exacerbated by a high degree of monopolistic or oligopolistic production.[2]That notwithstanding, exports still provided the foreign exchange used to pay for imports of capital goods that were essential for domestic investment.
Estimates say that Africa will account for 80 percent of the projected four-billion increase in the global population by the year 2100; the accompanying increase in its working-age population creates a window of opportunity, which if properly harnessed, can translate into higher growth and yield a demographic dividend. Analysts observe that the significant interaction between human capital and the magnitude of the demographic dividend suggests that improving and increasing access to education is critical to improve the productivity of workers and support a transition to higher valued-added sectors.[3]Moreover, structural transformation fostering a shift away from agriculture could help Africa reap its demographic dividend. As such, policies that remove impediments to private sector development and enable labour-intensive manufacturing could help position Africa to make the most of its resources.
The health of a population drives economic growth, and vice versa. Robust economic growth provides more fiscal space for public allocation of resources for social sectors and for prioritising healthcare. After all, it is estimated that Africa faces a financing gap for healthcare of US $66 billion per annum.[4]The existing—and widening—gap between the growth rate of Sub Saharan African (SSA) countries and other developing regions can be explained by various factors, foremost among them, health inequality. The region needs to engage in and encourage innovative and cost-effective health interventions that will help improve allocative efficiency and production of health, with the ultimate goal of making possible health-led economic growth and development.[5]Studies that explore the impact of healthcare on economic growth in Africa have established that both health expenditures and health outcomes have a direct and positive impact on economic growth. In particular, achieving reduction in maternal mortality, infant mortality and child mortality are all growth-friendly.[6]
Healthcare in Africa: An Overview
Countries in Africa continue to be plagued with poverty for a myriad reasons. Failing healthcare systems is key to why health outcomes in the continent tend to be low. For instance, SDG 3.1 calls for a reduction in the global maternal mortality rate (MMR) to less than 70 per 100,000 live births by 2030 and countries are expected to have an MMR of no more than twice the global average. Table 1 summarises trends in MMR from 2007-2017 for various United Nations Children’s Fund (UNICEF) regions.
Table 1: Trends in estimates of MMR—maternal deaths per 100,000 live births—2000-2017
Sub-Saharan Africa is trailing behind all other regions—despite a decline in MMR over the years, the region still recorded a high MMR of 533 per 100,000 live births in 2017. Moreover, West and Central African countries recorded the highest MMR in any of the years with 674 per 100,000 live births recorded in 2017.
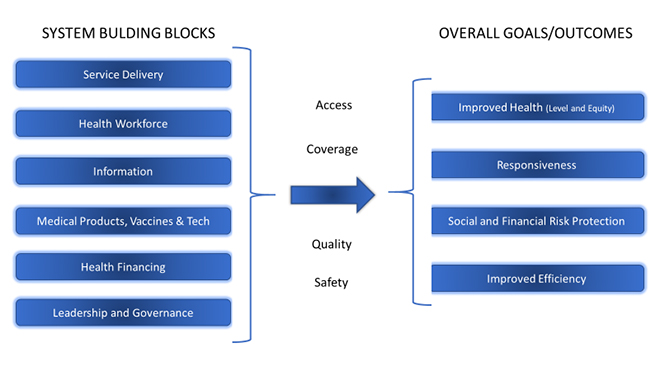
The World Health Organization (WHO) has identified six pillars that countries should focus on when improving their healthcare systems. (See Figure 1) A key concern of governments and other stakeholders who invest in health systems is how to tell whether and when the desired improvements in health system performance are being achieved.[8]Moreover, to achieve their goals, all health systems are required to carry out some basic functions, regardless of how they are organised: they have to provide services, develop health workers and other key resources, mobilise and allocate finances, and ensure health system leadership and governance.
Figure 1: WHO Health Systems Framework
Source: World Health Organisation
Some of the weaknesses can be attributed to challenges related to the six pillars, as illustrated in Figure 1.[9]Those issues are as follows:
Serious leadership and governance challenges. These include weak public health leadership and management; inadequate health-related legislations and their enforcement; limited community participation in planning, management and monitoring of health services; weak inter-sectoral action; horizontal and vertical inequities in health systems; inefficiency in resource allocation and use; and poor national health information and research systems.
Extreme shortage of health workers. The crisis is exacerbated by inequities in workforce distribution and brain drain, leading to the delivery of public health interventions to people in need being compromised, particularly in remote rural areas.
Rampant corruption in medical products and technologies procurement systems. Related issues include unreliable supply chains, unaffordable prices, irrational use, and wide variance in quality and safety—all contributing to a lack of access to essential medicines.
A dearth of information and communications technology (ICT) and mass internet connectivity. Moreover, there is a paucity of ICT-related knowledge and skills, limiting the capacities of national health management information systems (HMIS) to generate, analyse and disseminate information for use in decision-making.
Low investment in health. The manifold financing issues include a lack of comprehensive health financing policies and strategic plans, extensive out of pocket payments (OOP), lack of social safety nets to protect the poor, weak financial management, inefficient resource use, and weak mechanisms for coordinating partner support.
Lack of effective organisation and management of health services. Combined with the other challenges, this has led to the current situation where 47 percent of the population have no access to quality health services and 59 percent of pregnant women deliver without the assistance of skilled health personnel. In relation to water and sanitation, which contribute to reducing the burden of communicable diseases, 64 percent of the population lack sustainable access to improved sanitation facilities and 42 percent do not have access to an improved water source.
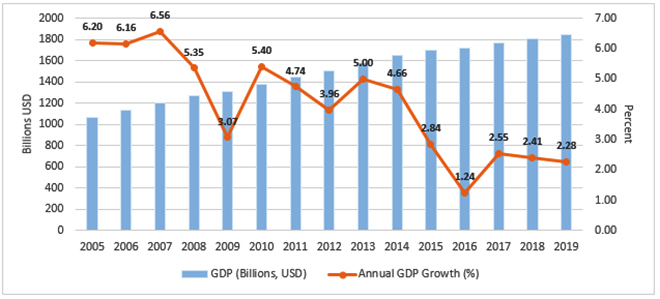
The World Bank, the Japan International Cooperation Agency (JICA), the Global Fund, the African Development Bank, and WHO[10]have noted that strong economic growth in Africa in recent years has helped reduce poverty to 43 percent of the population. Figure 2 shows the trend of economic growth in Africa in the last 15 years. Yet, as Africa’s population expands—it is estimated to reach 2.5 billion by 2050—the region faces the critical challenge of creating the foundations for long-term and inclusive growth. Many countries still contend with high levels of child and maternal mortality, malnutrition is far too common, and most health systems are not able to deal effectively with epidemics and the growing burden of chronic diseases such as diabetes. These challenges call for renewed commitments and accelerated progress toward Universal Health.
Figure 2: Economic Growth Trends in Sub-Saharan Africa
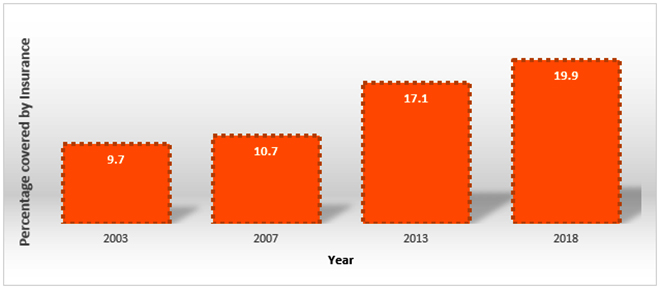
WHO has noted that Universal health coverage (UHC) means that all people and communities can use the promotive, preventive, curative, rehabilitative and palliative health services they need, of sufficient quality to be effective, while also ensuring that the use of these services does not expose the user to financial hardship. UHC is considered an effective investment since the prevention of malnutrition and ill health is likely to have enormous benefits in terms of longer and more productive lives, higher earnings and averted healthcare costs. Most African countries have integrated UHC as a goal in their national health strategies. Yet, progress has been slow in translating these commitments into expanded domestic resources for health, effective development assistance and ultimately equitable and quality health services and increased financial protection. For instance, when considering how protected citizens are against hardship while accessing healthcare services, one would consider looking at catastrophic health expenditures associated with OOP payments for health, reducing people’s ability to spend on other essential items, and impoverishing health expenditures associated with OOP payments for health that push people into poverty.[12]Health insurance cover also seeks to bring to light citizens who have some form of pre-paid cover, which provides a level of reduced financial risk of being exposed to large healthcare costs. Figure 3 shows insurance coverage in Kenya where there has been a significant growth; however, out of the 47.8 million national population for the year 2018, 80.1 percent are not covered by any form of health insurance.
Figure 3: Trends in Health Insurance Coverage, Kenya (Various years)
The disease burden in Africa continues to increase. This includes both the communicable disease burden and the increasing non-communicable diseases that are mainly lifestyle diseases. With this increase, governments have had to correspondingly raise their spending on healthcare. Table 2 summarises the health financing profile for Sub-Saharan Africa compared to the whole world for the year 2016.
Table 2: Total Health Spending, SSA (2016)
Indicator
Total
Sub-Saharan Africa
Health spending per person ($USD)
1,077 (1,058 to 1,096)
80 (75 to 86)
Health spending per person ($PPP)
1,400 (1,368 to 1,432)
199 (186 to 214)
Health spending per GDP (%)
8.6 (8.4 to 8.7)
4.1 (3.9 to 4.3)
Government health spending per total health spending (%)
74.0 (72.5 to 75.5)
36.8 (34.0 to 39.8)
Out-of-pocket spending per total health spending (%)
18.6 (18.0 to 19.4)
31.5 (27.3 to 36.3)
Prepaid private spending per total health spending (%)
7.2 (6.7 to 7.8)
17.9 (14.5 to 22.3)
Development assistance for health per total health spending (%)
0.2 (0.2 to 0.2)
14.0 (13.1 to 14.9)
Source: Institute for Health Metrics and Evaluation[14]
In 2016, health spending as a percentage of GDP in Sub-Saharan Africa was less than half that of the world, while development assistance as a percentage of total health spending was 14 percent as compared to the world at 0.2 percent. This clearly shows that governments in countries in sub-Saharan Africa allocate less money to health and, thus, receive more external funding towards health. Further commitment to financing UHC would be demonstrated if the government could honour the Abuja obligation of allocating at least 15 percent of the national budget to the health sector.
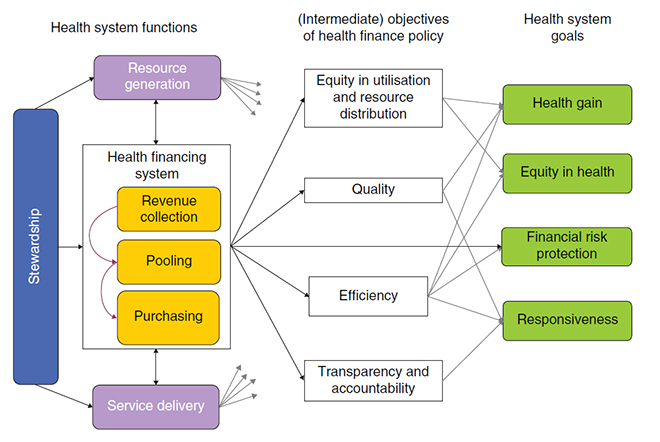
Figure 4: Health System Financing and Goal Attainment (2018)
Figure 4 gives a snapshot of health financing—how revenues are raised, pooled and used in an efficient manner to produce quality healthcare services that benefit the citizens equitably, all while protecting the citizens from financial hardships as they access healthcare services.
Use of economic evaluation or cost effectiveness in decision-making
Many decision-makers undertake cost-effectiveness analysis (CEA) when evaluating interventions and developing evidence-based clinical guidelines. However, the recommendations arising from cost-effectiveness analysis are often not implemented as intended. A fundamental reason for this implementation failure is that CEA assumes a single constraint, in the form of the budget constraint, whereas in reality decision-makers may be faced with numerous constraints that inhibit change in the health system.[16]In case of multiple constraints, the default decision rules of cost effectiveness do not apply anymore and decision rules become more complex.[17]As a solution to this, some studies have advocated the use of mathematical programming to arrive at an optimal allocation of resources in the presence of multiple constraints.[18][19]In these studies, numerous constraints were considered, varying from demand and supply constraints to equity constraints. A drawback of mathematical programming is that the analytical capabilities for these techniques are substantial and it is difficult to translate insights from such studies—in which a high degree of intervention is included—to simple cost effectiveness studies where only a few interventions are compared, and central outcomes expressed in incremental cost effectiveness ratios (ICER).
Moreover, CEA can be used to come up with a list of interventions or “benefits package” that will be financed publicly. Patients needing an intervention not in the benefit package will have to pay out of pocket, or else go without it. CEA can be operationalised with existing data on costs and effects of different interventions. There are existing cost-effectiveness estimates for a large number of interventions, and in different settings. This data can be used to rank interventions in descending order of cost-effectiveness, estimate the number of people likely to need each intervention, and then keep adding interventions to the benefit package until the budget is exhausted. However, the benefits package only cover those people who require a highly cost-effective intervention, or whose private resources are large enough to enable them to finance a relatively cost-ineffective intervention. This group will likely include a disproportionately large number of relatively well-off people.
The results of cost-effectiveness studies have been used to inform decision-making regarding healthcare input constraints. However, the issue of opportunity costs expressed in health foregone becomes even more important as they differ between healthcare inputs. The presence of healthcare input constraints influences the decision rules of cost effectiveness, and offered practical solutions to re-analyse and interpret cost effectiveness studies in such circumstances.[21]In standard cost effectiveness analyses, it is implicitly assumed that opportunity costs are equal everywhere in the healthcare sector and therefore it does not matter from which healthcare inputs the resources are drawn from. However, in the presence of healthcare input constraints, it is important to realise from where health care resources are being drawn from. Consequently, conventional ICERs need to be adjusted by taking into account that some costs will have larger displacement effects in terms of health forgone than other costs.
Finally, in low and middle income countries (LMIC) there is often a lack of supply of skilled doctors and nurses which might influence costs and health effects of delivering a particular healthcare technology.[22][23]Increasing the size and skills of the workforce is often not that easy[24]and raising wages to increase the workforce in low income countries might have limited success as it is difficult to compete with wages in Western countries.[25]In these settings, human resource constraints limit the usefulness of CEA studies for decision-makers as applying the standard decision rules could result in suboptimal decisions.
Conclusion
Africa’s healthcare system faces challenges pertaining to leadership and governance, the healthcare workforce, medical products and technologies systems, HMIS and ICT, healthcare financing and overall coordination and management of health services. In turn, low-quality healthcare results in increased disease burdens and impedes the attainment of universal health coverage.
Poor health outcomes will persist in Africa as long as healthcare systems are not able to carry out even their basic functions. Even as governments look forward to ensure that all individuals access quality healthcare services without suffering financial hardship, there is a need for decision-makers to prioritise use of evidence to inform investment in health; in addition, prioritisation of health should be reflected in the budget in line with achieving sustainable financing for health.
About the Authors
Daniel Mwai is a health economist and a lecturer of health economics at the University of Nairobi Kenya. He has over 14 years of local and international experience guiding the adoption of policies across all levels of the health system.
Theresa Ndavi is a senior economist at the Palladium Group’s Health Policy Plus Project. She has over seven years of expertise working across Africa in statistics and economic modelling for health, social and development policy.
[2]Overseas Development Institute. Industrialisation in Sub-Saharan Africa.Briefing Paper ODI(1986).
[3]Drummond, P., Thakoor, V., and Yu, S. Africa Rising: Harnessing the Demographic Dividend.IMF Working PaperWP/14/143. (2014). International Monetary Fund, African Department.
[5]Ogunleye, E.K. Health and Economic Growth in Sub-Saharan Africa.AERC Research Paper284 (2014). Africa Economic Research Consortium. Nairobi.
[6]Some, J., Pasali, 2., and Kaboine, M. Exploring the Impact of Healthcare on Economic Growth in Africa.Applied Economics and FinanceVol. 6, No. 3. (2019). Pp 45-57. Redfame Publishing.
[7]World Health Organisation.Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. (2019) WHO. Geneva.
[10]World Bank, JICA, The Global Fund, African Development Bank and World Health Organisation.Universal health coverage in Africa: a framework for action. [Online]Joint 2016 TICAD conference working paper. (2016)
[11]World Bank. World Development Indicators. The World Bank Group.
[18]Epstein, D. M., Chalabi, Z., Claxton, K., & Sculpher, M. Efficiency, Equity, and Budgetary Policies.Medical Decision Making, 27(2), 128–137 (2007).
[19]Feenstra, T. L., van Baal, P. M., Jacobs-van der Bruggen, M. O., Hoogenveen, R. T., Kommer, G. J., & Baan, C. A.Targeted versus universal prevention. A resource allocation model to prioritize cardiovascular prevention.Cost Effectiveness and Resource Allocation, 9(1), 1–11. (2011)
[22]Fulton, B. D., Scheffler, R. M., Sparkes, S. P., Auh, E. Y., Vujicic, M., & Soucat, A. (2011). Health workforce skill mix and task shifting in low income countries: A review of recent evidence.Human Resources for HealthVol. 9, Issue 1, p. 1(2011) BioMed Central.
[23]WHO | The World Health Report 2006 – working together for health. (2013). WHO.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Theresa Ndavi is a senior economist at the Palladium Groups Health Policy Plus Project. She has over seven years of expertise working across Africa in ...

 PDF Download
PDF Download