The Role of Gender Equity in Reducing Malnutrition: The View from South Asia
This brief analyses the correlation between gender-based inequities and malnutrition. It highlights the case of South Asia, and uses as a backdrop the compounded challenges resulting from the COVID-19 pandemic. The authors review existing literature on the subject and cull patterns, with the aim of outlining recommendations for countries in the region for bridging interrelated gaps in gender parity and nutrition.
Attribution:
Shaonli Chakraborty, et al., “The Role of Gender Equity in Reducing Malnutrition: The View from South Asia,”ORF Issue Brief No. 578, September 2022, Observer Research Foundation.
Introduction
Gender-based inequities remain a massive challenge in many parts of the world, and women and girls continue to face discrimination throughout the different stages of their lives. They have less access to education, healthcare, and nutrition, they face the threat of violence, and have a poorer quality of life, overall.[1]The inequities that girl children face can have cascading effects later in their life: those who are deprived of quality education grow up having limited access to income opportunities and being denied financial autonomy.[2]Poor access to healthcare services leads to worse health outcomes, increasing greater susceptibility to infections and diseases that increase morbidity and mortality.
This brief aims to highlight the correlation between gender inequities and the persistence of malnutrition in women and children. It is these social determinants that have led to inequality and power imbalance between genders, in turn impacting food production and eating habits. Despite women playing the most crucial role in household nutrition, they are often found at the bottom rung of the family when it comes to nutrition.[3]
The COVID-19 pandemic only exacerbated the problem. More than two years since the World Health Organization (WHO) declared the pandemic, the global population is still reeling from the myriad health challenges brought about by the outbreak. Little attention, however, has been paid to its impacts on maternal and child malnutrition. Indeed, even prior to the pandemic, limited progress was being made towards achieving the global nutrition targets. Going by the findings of theGlobal Nutrition Report 2021, the targets now appear to have become even more elusive, given how the pandemic had pushed an additional 155 million people into extreme poverty.[4]
With poverty and illness interlocked in a vicious cycle, loss of livelihood has impacted people’s food habits and, thereby, their nutritional status. Women have to shoulder the dual burden of their gender roles along with more hours of unpaid labour.[5]Compounding the challenges is the climate crisis, which affects food production, access, and affordability, and in turn impacting women the most,[6]especially among the rural and urban poor, the marginalised communities, and those with disabilities.
This brief examines how gender inequities contribute to malnutrition. The rest of the brief outlines the cycles of malnutrition, analyses the nutrition status of women and children and, focusing on South Asia, explores programmes and policies that aim to improve nutritional outcomes.
The Cycles of Malnutrition
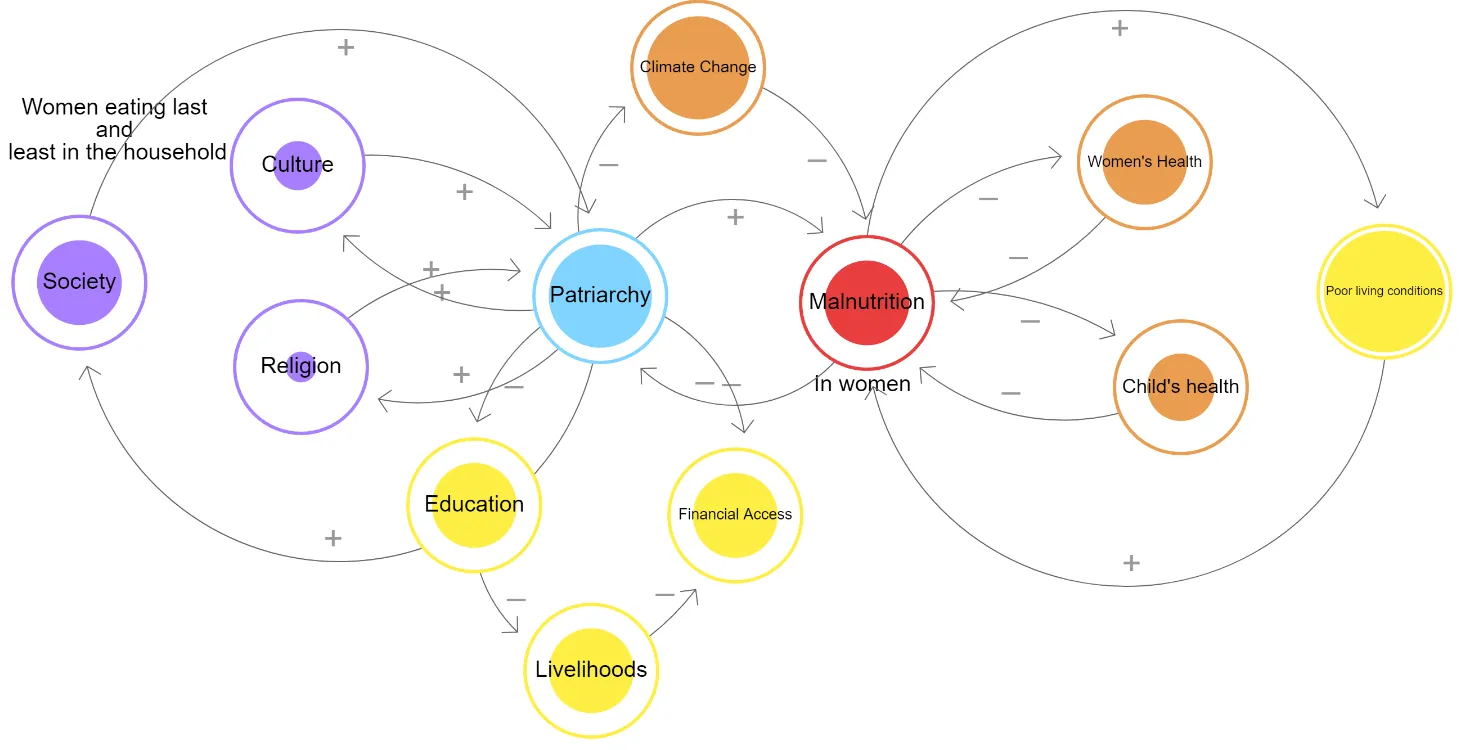
In Figure 1, the authors have drawn a causal loop diagram to demonstrate the factors impacting, and in turn getting impacted, by malnutrition. Each of these factors needs to be understood if adequate and appropriate policy interventions are to be formulated to improve health outcomes for women.
Figure 1: Gender Inequity and Malnutrition: The Causal Loop
Source:Authors’ own
The diagram illustrates the correlations between key factors driving gender inequities, and malnutrition. Norms and practices that worsen gender inequity have a negative impact on many aspects of women’s lives, such as access to education, job, or income, rendering them dependent on men for even basic survival needs. With limited or no control over their own bodies, health, and nutrition, women continue to bear the brunt of poor health outcomes. This affects the health and well-being of their children, pushing the family into intergenerational, chronic malnutrition.
Studies have found that in South Asian countries, conditioning of women starts right from childhood, where putting others’ needs before their own is rewarded.[7]While the woman shoulders the responsibility of cooking and feeding the family, she herself seldom gets to eat on time, nor adequately. Her economic growth is tethered to her education, which is disregarded easily, especially when a choice has to be made between her getting educated and her close male relatives, be they a sibling or spouse. Therefore, it is not too difficult to understand the rising numbers of malnutrition across the globe, both of women and children. Iron deficiency anaemia adversely affects maternal and foetal well-being and is linked to increased morbidity and foetal death.[8]Infants and children with iron deficiency anaemia are at risk of developmental difficulties involving cognitive, social-emotional, and adaptive functions.[9]
The other side of malnutrition is obesity. India’s National Family Health Survey-5 (NFHS-5), released in May 2022, notes that 4.2 percent of children under five in urban India are overweight.[10]This corroborates the observations of a paper on ‘Child Obesity and Urbanisation in India’ (2021) that pointed out the rise of child obesity in affluent families – where women are presumably much more aware – due to poor lifestyle and diet choices, such as high-sugar drinks and processed snacks.[11]
Widening Gender Gaps: Focus on South Asia
South Asia is the second-lowest performing region in theGender Gap Report 2021, with only West Asia and North Africa scoring worse.[12]Among countries of the region, India is now one of the worst performers with a rank of 140 out of 156 countries, while Bangladesh stands at 65, Nepal at 106, Bhutan at 130, and Sri Lanka at 116. (Only Pakistan at 153 and Afghanistan at 156, are behind India.) The same report noted that South Asia is the region that regressed the most this year, with a gender gap 3.4 percentage points wider than one year ago.[13]Data also shows that it will take 135.6 years to bridge the gender gap worldwide and that the pandemic has impacted women more severely than men.
A 2012 World Bank report noted that gender was the basic, and perhaps the most critical determinant of nutrition outcomes.[14]Even a decade later, gender inequities continue to prevail among South Asian countries. The women’s low status, especially in the household, directly impacts her ability to make decisions regarding not only her own food intake but also that of her children. Decisions around exclusive breastfeeding, initiating and maintaining adequate complementary feeding, remain with other family members, especially the spouse and/or the household’s male head.
Research by the World Institute of Development Research has noted that despite the significant contribution women make in food production (especially agriculture-related work), their earnings remain low, and are almost entirely invested back into the family.[15],[16]They therefore have limited or no autonomy; their awareness and access to information remains poor, especially regarding choice of diet, both for themselves and their children.
There are various women’s empowerment-related indices measuring the correlation between women’s status and various developmental outcomes related to food security, gender equality, agency, and inclusion in various sectors. The women’s empowerment in agriculture index (WEAI) of the International Food Policy Research Institute (IFPRI) links women’s empowerment, food security, and agricultural growth. It measures the role and extent of women’s engagement in the agriculture sector in five domains: decisions, access, control leadership, time engagement, and women’s empowerment within their households. Studies using the index suggest that women’s role in agriculture is largely undervalued, though they contribute significantly to this sector as wage labourers. They are denied market and other forms of economic access, and mostly remain invisible. The studies found that malnutrition, which often manifests as anaemia, is widely prevalent among women farmers and wage labourers.[17]There is also the Women Empowerment Index (WEI) and the Women Economic Empowerment Index (WEEI) of the UN which help measure, track and prioritise gender-responsive projects both by the private and public sector.[18]These indexes need to be further used to gather data and build evidence to improve and support inclusion of women.
Nutrition Status of Women and Children
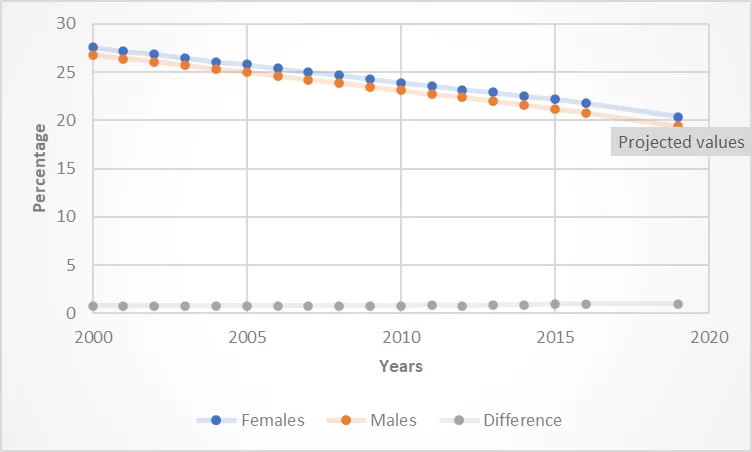
A notable proportion of both men and women in South Asia are underweight. However, theGlobal Nutrition Report 2021notes that while this condition has been reducing since 2000, the gap between the genders on this score has not shrunk; instead, it has widened in the last few years (see Figure 2).
Figure 2: Underweight Population in South Asia
Source:GNR (2021)
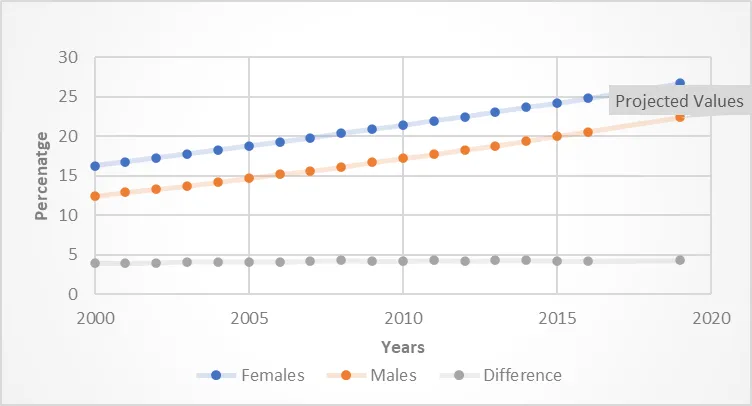
There is also evidence that while the number of underweight women has been decreasing, the number of those who are overweight has been increasing (see Figure 3).
Figure 3: Overweight Population in South Asia
Source:GNR (2021)
The charts reveal that there are more women than men in both the overweight and underweight categories, and that the gap between the genders in both cases is increasing. The same report notes that South Asian countries have made some progress in reducing childhood stunting, increasing breastfeeding, and managing childhood obesity. However, they have seen little success in reducing anaemia, and certain countries continue to struggle with low birth weight as well as obesity. Anaemia alone has a severe impact on the health and economy of any country. A report by Niti Aayog has noted that “physical and cognitive losses due to iron deficiency anaemia (IDA) costs the developing countries up to 4.5 percent loss in GDP per annum, which is 1.18 percent of GDP in India, thereby stalling social and economic development. Women under the reproductive age group are most vulnerable when it comes to IDA.”[19]
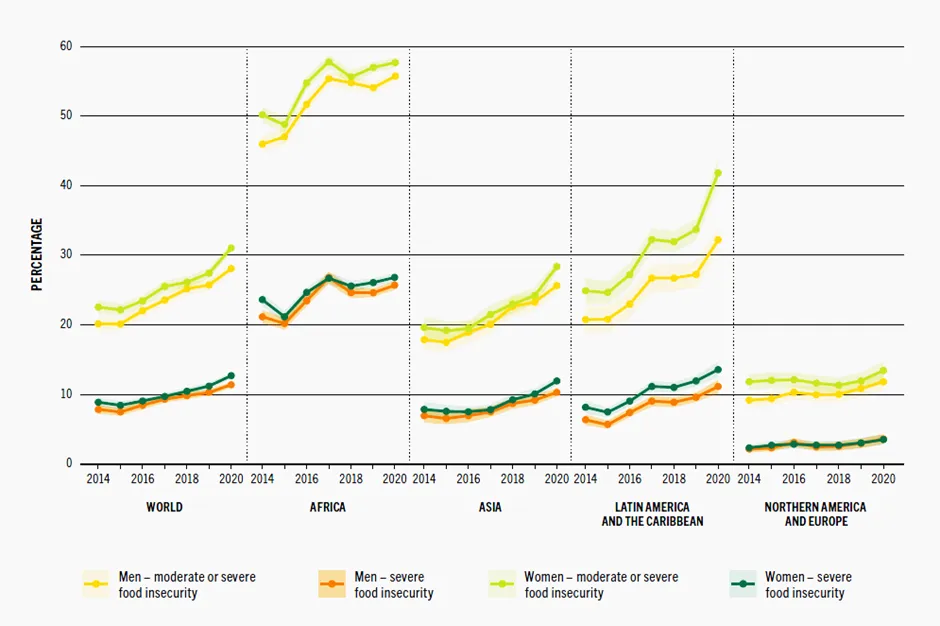
The UN’sState of Food Security and Nutrition in the World, 2021report has highlighted that more than half of the world’s undernourished people – 418 million – are to be found in Asia, and that women remain worse off than men.[20]While food insecurity is higher among women than men in many parts of the globe, the numbers appear to be worse in South Asia.
Figure 4: Global Prevalence of Food Insecurity
Source:Adopted from the FAO SOFI (2021)
Despite interventions by local governments, and support from organisations such as WHO as well as the private sector, tackling malnutrition remains an uphill task. The latest figures show that current strategies and policies are not able to fully address its root causes, nor influence behavioural norms and practices to improve nutrition levels and address the lack of gender parity.
Programmes and Policies in South Asian Countries for Women’s and Children’s Nutrition
South Asian countries have in place various policies, programmes, strategies and action plans aimed at improving the nutritional status of women and children. These include legislating the mandatory iodisation of salt, and issuing dietary guidelines. Among the international programmes is the World Bank’s South Asia Food and Security Initiative (SAFANSI), launched in 2010, designed to address chronic malnutrition issues through measurable improvements in food and nutrition security across the region.
The following paragraphs describe the most significant steps taken by individual countries so far:
India
The Public Distribution System (PDS)—the government-controlled distribution of food grains to poor families launched in the 1970s—remains one of India’s key responses to food insecurity and hunger. The expansion in 2003–2006 of the Antyodaya Anna Yojana scheme also included provision of highly subsidised food and goods to senior citizens and pensioners over 60 years, as well as widows and people suffering from disease or infirmity.[21]
Meanwhile, the Poshan Abhiyaan was launched in 2018 as a flagship initiative to improve nutritional outcomes for children, pregnant women, and lactating mothers. Its key strategy was the Jan Andolan, aimed at influencing behaviours around nutrition through effective communication.
In February 2021, Poshan 2.0 was launched to deepen interventions in maternal and child nutrition. While the Poshan Abhiyaan focused on community action to reduce malnutrition (especially stunting and wasting) and improve infant and young child feeding practices, Poshan 2.0 is an integrated nutrition support programme (Saksham Aanganwadi) aimed not just at content creation, but also delivery of services through existing infrastructure.[22]
Another centrally sponsored scheme, the Mid-Day Meal (MDM) scheme, which has existed in the country for decades, makes freshly cooked lunch available for free to government school students. A study by Chakrabarti et al. (2021) reported that children born to mothers who had consumed the mid-day meals while they were in school themselves, were on average healthier than those born to mothers who had not. The height-for-age (HAZ) z-score among children in the first category was greater (+0.40 standard deviation) than for those in the second.[23]Previous econometric evaluations of the MDM scheme have also noted positive associations with beneficiaries’ school attendance,[24]learning achievement,[25]and resolving hunger.[26]
Bangladesh
Bangladesh has multiple policies and plans to combat malnutrition, including its National Nutrition Policy (2015) and its Health, Nutrition and Population Strategic Investment Plan (2016-2021). The former, with its closely linked National Plan of Action for Nutrition (NPAN) is designed to improve overall nutrition of the population, while the latter aims at quality and equitable healthcare through universal health coverage.[27]
Pakistan
In 2018, Pakistan launched the Pakistan Multi-Sectoral Nutrition Strategy (2018-2025) to reduce malnutrition through an enabling federal policy environment, capacity-building initiatives, communication, advocacy, and public education, and implementation of a national monitoring and evaluation plan to assess progress.[28]
Afghanistan
Afghanistan, ravaged by war and uncertainties, has faced severe challenges in planning and executing sustainable policies to improve the nutritional status of its population. Its political will to achieve this goal, however, has to be admired. Its initial nutrition policies focused on health interventions through its various facilities, which aimed at improving antenatal care, providing micronutrient supplements, and offering nutrition education. Providing care and treatment of acutely malnourished children both at the facilities and in the household was an integral part of its policy.
Subsequently, the country has invested in developing several nutrition-related policies and strategies, including the prevention and control of vitamin and mineral deficiencies (2009), and the infant and young child feeding strategy (2009). The Nutrition Action Framework and the Afghanistan Food Security and Nutrition Agenda have since been developed, which prioritise designing a multi-sectoral action plan to improve nutrition.[29]
Sri Lanka, Bhutan, and the Maldives
In Sri Lanka, Bhutan, Nepal, and the Maldives, the policy focus has been on ensuring food security, micronutrient fortification, and education on diet diversity as well as infant and young child feeding practices.
Social protection is a key enabler for social and economic empowerment of non-cisgender communities (LGBTQA). Some countries in South Asia, such as India and Pakistan, have progressive protection laws enabling social inclusion and poverty reduction of these communities, and thereby improving their food security. Countries such as Nepal and Bangladesh have initiated social identity programmes to improve the status of trans people. Overall, however, the policies and programmes for these sections remain inadequate and fragmented.
Recommendations and Conclusion
This brief offers the following recommendations to address the twin challenges of gender inequity and malnutrition:
Continue supporting education for women, with financial aid where necessary, to ensure their employability and/or capacity for entrepreneurship.
Review current pay scales and encourage both formal and informal employers to reduce the pay gaps between men and women.
Develop and implement country-level policies that further empower women and girls.
Redesign behaviour change communication strategies related to essential nutrition actions (such as healthy maternal nutrition, exclusive breastfeeding, and timely and adequate complementary feeding) to target key decision-makers in families and communities instead of only young wives and mothers.
Continue investing in country-wide interventions to address systemic and normative transformations, and make data assessing the results, available to the public.
Invest in further research on the impact of malnutrition on LGBTQ communities.
WHO’s Global Nutrition Goals are targeted to be achieved by 2025. More effective efforts are needed to correct nutritional outcomes, be it childhood stunting and wasting, or anaemia in women of reproductive age. In South Asian countries, gender biases continue to significantly undermine nutritional outcomes for women and children. Women continue to have little autonomy, if at all, in meeting their own nutrition needs and those of their children. Women and children from poor and marginalised communities continue to be severely affected by malnutrition. Similarly, non-cis-gender communities, including trans people, continue to be among the most vulnerable.
The disparity in livelihood options between the genders, as well as the pay gaps, create significant barriers to food security, which in turn lead to malnutrition. The interlocking of poverty and ill-health contributes to reduced income, with its inevitable consequences on nutrition. Unless every household invests in nutritious food, the vicious cycle of poverty, illness, and thereby reduced income—and poor decision-making thereafter which sacrifices nutrition—will continue to impede the health and economic growth of the region.
Comprehensive policies that impact the health and nutrition outcomes of women, children, and minority communities, require a multi-pronged approach, going beyond behaviour change communication. Policies and programmes should focus on creating inclusive livelihood opportunities and workspaces, especially for women and trans people, ensuring financial inclusion (which will result in poverty reduction), economic empowerment, and protection from violence. Existing policies in most of South Asia are underperforming or fragmented. Proper interventions will ensure access to livelihood, financial security, and overall autonomy for women.
There is also a strong need for strategic interventions that address ingrained gender biases, gender-based discrimination, and violence driven by patriarchal norms and practices. Instead of designing interventions and communications targeted only at women, policies and programmes should be designed to educate and guide other stakeholders. This will lead to improved access to resources, opportunities, critical information, and skills that will act as enablers in reducing malnutrition among vulnerable groups.
[5]Gaëlle Ferrant, Luca Maria Pesando and Keiko Nowacka, “Unpaid Care Work: The missing link in the analysis of gender gaps in labour outcomes,” OECD Development Centre, December 2014.
[8]Noran M Abu-Ouf, and Jan Mohammed M, “The Impact of Maternal Iron Deficiency and Iron Deficiency Anaemia on Child’s Health”,Saudi Medical Journal36 (2015): 2, pp 146-149. doi:10.15537/smj.2015.2.10289.
[9]Bener, A, M Kamal, HZ Bener, and D Bhugra, “Higher Prevalence Of Iron Deficiency As Strong Predictor Of Attention Deficit Hyperactivity Disorder In Children”.Annals of Medical And Health Sciences Research4 (2014): 9, pp 291. doi:10.4103/2141-9248.141974.
[15]Nira Ramachandran,”Women and Food Security In South Asia: Current Issues And Emerging Concerns”,Econstor(2006). doi:10.1.1.395.8559.
[16]Janna Visser and James Wangu, “Women’s Dual Centrality In Food Security Solutions: The Need For A Stronger Gender Lens In Food Systems’ Transformation”,Current Research In Environmental Sustainability3 (2021): 100094. doi:10.1016/j.crsust.2021.100094
[23]Suman Chakrabarti, Samuel P Scott, Harold Alderman, Purnima Menon and Daniel O Gilligan, “Intergenerational nutrition benefits of India’s national school feeding program”,Nature Communications12 (2021): 4248. doi.org/10.1038/s41467-021-24433-w
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Shaonli Chakraborty is a development professional with over 20 years of work experience in various countries in South Asia and Africa. She has led and ...
Piyasree Mukherjee is a social development professional and public health nutrition specialist with a career spanning over two decades. Her expertise lies in programme and ...
Ravneet Kaur is a young professional with key interests in public health nutrition food policies and health systems strengthening. She is a public policy graduate ...
Samana Shreedhar graduated with a Bachelors degree in Business and Environmental Science from James Cook University (Singapore) in 2019. She is currently a research fellow ...

 PDF Download
PDF Download