The Impact of COVID-19 on Children and Adolescents: Early Evidence in India
This brief collects and analyses current evidence in India regarding the impact of COVID-19 on the health and well-being of children (5-9 years) and adolescents (10-19). Using the ‘snowball retrieval’ strategy, the authors identified peer-reviewed studies, reports and government articles published between January 2020 and February 2021 that were relevant to the research question. The brief finds that not only are children and adolescents highly vulnerable to the impacts of the pandemic, but that these ramifications are manifold and require immediate attention. The analysis highlights the disproportionately greater vulnerability of girls in the areas of education, domestic violence, child marriage, domestic workload, and mental health.
Attribution:
Attribution: Deepika Bahl, Shalini Bassi, and Monika Arora, “The Impact of COVID-19 on Children and Adolescents: Early Evidence in India,” ORF Issue Brief No. 448, March 2021, Observer Research Foundation.
Introduction
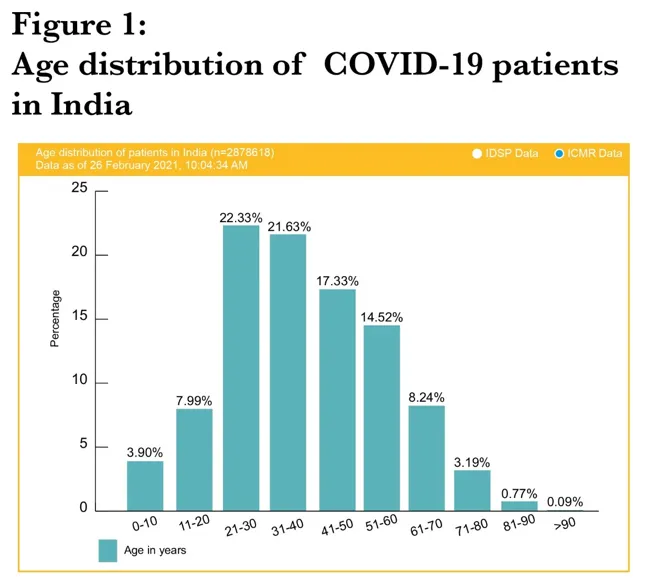
At the time of writing this brief, there were 111 million confirmed cases of COVID-19 across the globe; the death toll was at 2.46 million. In India, 11,005,850 million confirmed cases of COVID-19 and 156,418 deaths have been recorded.[1]Stratification by age shows that the prevalence of COVID-19 was higher among those between 21-30 years, and lowest among children (0-10) and adolescents (11-20).[2](See Figure 1)
Figure 1: Age distribution of COVID-19 patients in India
As of September 2020, children under 18 years comprised 8.5 percent of all reported COVID-19 cases in the world.[4]In the United States (US), among the worst-hit by the pandemic, children (0-20 years) from 49 states comprised 13.1 percent of all COVID-19 cases as of February 2021.[5]These numbers, however, were heavily dependent on testing criteria; in many cases, testing was done only on individuals who were symptomatic or required hospitalisation—this happens less often for children and adolescents.[6]
Research across the globe has shown that children and adolescents who are infected with COVID-19 exhibit fewer symptoms, are less likely to become severely ill when they do get infected, and have lower chances of transmitting the virus than adults.[7],[8],[9]To be sure, there is contrary evidence from South Korea, for example, which suggests that adolescents (10-19) could spread the novel coronavirus as virulently as adults.[10]A study in the US found that children younger than five years with mild to moderate COVID-19 have a high amount of SARS-CoV-2 viral RNA in their nasopharynx compared with older children and adults.[11]
In India, despite relatively low rates and varied evidence, it is a growing concern that children and adolescents be protected from COVID-19 as they constitute a large proportion of the population.[12]Globally, lockdown measures that were imposed in the initial onslaught of the pandemic have affected children and adolescents’ health and well-being, their learning, and the economic security of their families. This brief analyses the consequences of the COVID-19 pandemic—and the prolonged lockdown, including of schools—on the children and adolescents of India.
Methodology
The authors of this brief searched and reviewed published articles in peer-reviewed journals that assess the effects of COVID-19 on children and adolescents’ health and well-being. Using the ‘snowball search’ strategy, the authors mined peer-reviewed articles, reports, and government websites for evidence from January 2020 to February 2021.[a]
Findings and Analysis
While countries are battling the pandemic and working to save lives and livelihoods, children’s and adolescents’ needs may not immediately appear to warrant significant attention. Yet, the measures adopted to curtail the spread of the new virus (including closure of schools, restrictions on movement, physical distancing, mask-wearing, and restricted social gatherings) can have massive adverse impacts on children and adolescents.
Education and learning outcomes
A rapid systematic review published in April 2020 inLancetestimated that school closure alone could reduce COVID-19-related mortality by 2 to 4 percent.[13]India closed down its schools on 16 March 2020—one of the first countries in the world to do so—[14]and moved to online learning as an emergency measure. Following the closure of schools, virtual platforms have been used in all grades to continue with children’s schooling.[15]Early analyses of India’s experience have found that the country’s socio-economic inequalities are influencing the effectiveness of virtual learning (or lack of it). There are widespread challenges facing significant proportions of the school-age population, including unavailability of smartphones and computers, unreliable internet connection (if at all), lack of technology skills,[16]and lack of electricity.[17][18]
A survey of 23 states among school children (grades 1 to 12) conducted in April 2020 found that only 43.9 percent of them have access to smartphones, another 43.9 percent of them have access to basic phones, while a significant 12.0 percent do not have access to either smartphones or basic phones.[19]In Maharashtra, for example, only 50 percent of public school students from classes I to VIII could access digital learning.[20]Around 59.8 percent of public school students had access to smartphones with internet, and among them only 30 percent were using the state’s online platform, DIKSHA (Digital Infrastructure for Knowledge Sharing).[b],[21]Of those who are unable to access online learning, 72.2 percent of their parents do not have the digital skills to access the state home package, and 66.4 percent of families do not have access to smartphones. The availability of desktops and laptops among students was negligible at 0.8 percent.[22] Teachers also faced challenges due to their low level of digital literacy.[23],[24]
The United Nations (UN), in a report issued in August 2020, warned that prolonged school closure could result in a higher incidence of dropouts: 23.8 million additional children and youth (from pre-primary to tertiary) may drop out or not have access to a school in 2021.[25]The incidence of dropouts has been found to be higher among girls, especially those living in poverty, those with disabilities, or living in the rural regions. Even before the pandemic, millions of girls across India were already struggling with poor-quality education, unable to meet minimum proficiency in basic reading and mathematics, and least of all, secondary level skills they need to be able to have higher chances of leading a productive adult life.[26]According to the National Family Health Survey (NFHS-4), 7.3 percent of girls 6-9 years never attended school; the proportion is 3.6 percent for those 10-14, and 6.6 percent for those 15-19. Among boys, 6.9 percent of 6-9 year-olds never attended school; the proportion is 3.2 percent for 10-14 years, and 4.3 percent for those 15-19.[27]The data indicates that girls were already more vulnerable compared to boys even before COVID-19. Global evidence shows that during previous periods of disease outbreaks like Zika, SARS and Ebola, adolescent girls are more vulnerable due to lost earnings and education, increased vulnerability to gender-based violence, and unintended pregnancy.[28]
The government of India has taken steps to respond to the pandemic’s fallout on education: it released a set of guidelines for online education, called “Pragyata”,[29] and ordered for the use of DIKSHA platform for all states and union territories to enable learning at home through innovative state programmes. The State Departments of Education have also taken certain steps: in the Andaman and Nicobar Islands, for example, the education department has initiated home-based alternative learning methods for Class II to XII students by utilising channels such as the local Doordarshan. In Andhra Pradesh, meanwhile, online platforms like YouTube, as well as other avenues like a toll-free number, were introduced for quality transactions in classrooms.[30]
Child marriages
India has declared its commitment to achieve Sustainable Development Goal (SDG) 5 on gender equality[c]and, in particular, target 5.3 which calls for eliminating all harmful practices such as child, early and forced marriage; and female genital mutilation.[31]Over the years, the government has taken measures to eliminate child marriages through policies, laws and flagship programmes—among them, the National Population Policy (2000),[32]National Youth Policy (2014),[33]National Policy for the Empowerment of Women,[34]Prohibition of Child Marriage Act (PCMA), 2006,[35] Scheme for Adolescent Girls (SAG),[36]Rashtriya Kishor Swasthya Karyakram (RKSK),[37]and various national and state-level conditional cash transfer (CCT) programmes for girls.[38]Civil society organisations have also initiated their own programmes.
Yet the practice of child marriage has yet to be eliminated. In 2015-16, among adolescents in India (15-19 years), 2.6 percent of girls got married at the age of 15 and among 20-24 years, 26.8 percent of girls got married before 18.[39]Though these numbers have declined compared to the findings of NFHS-3,[40]evidence shows a continuing substantial burden. During the lockdown, the anti-child marriages programmes were disrupted. Research has shown that a mere one-year delay in these measures, not only in India—compounded by the economic downturn—could result in 13 million more child marriages over the next decade (2020-2030) across the globe.[41]
The risk of child marriages has heightened as a result of the pandemic’s economic fallout, as vulnerable households could be forced to adopt coping mechanisms. They would need to find alternative sources of income or else reduce their expenditure by reducing the size of the family and marrying off their child.[42]
According to data reported by ChildLine, a nodal agency of the Union Ministry of Women and Child Development protecting children in distress, out of 92,203 interventions, some 5,584 during the lockdown (35 percent) were related to child marriages. Of this number, 97 percent were minors (18 years and below) and 91 percent were girls.[43]In a study conducted in four states (Jharkhand, Chhattisgarh, Odisha, Bihar) among adolescents (10-19 years),[d]8 percent of the respondents have heard of an incidence of child marriage in their neighbourhood since the beginning of the pandemic. Two-thirds of adolescents reported that their family members were planning for their marriage and their chances of getting married early have increased; the proportion was higher among girls.[44]
In Madhya Pradesh, the recorded number of child marriages jumped from 46 cases between November 2019 and March 2020, to 117 cases in the shorter period of April to June 2020. Similarly, 18 cases of child marriages were reported in Chhattisgarh in the five months before the COVID-19 lockdown, but during the first three months of the lockdown, the number increased to 58.[45]
Domestic violence and other crimes
Analysts have identified multiple factors responsible for the alarming rise in the incidence of domestic violence at the time of COVID-19. These include health anxieties, financial difficulties, confinement in homes, and lack of mobility.[46],[47] In 2020, India’s children’s helpline, ChildLine, received 92,000 calls reporting child abuse and violence; during the lockdown, within only eleven days, the helpline logged one-third of this number.[48]
There has also been an increase in cybercrimes against children, including cyberbullying, especially in urban areas. Current analyses attribute children’s vulnerability to their heavy use of the internet and social media.[49]There is ample evidence that cyberbullying creates a significant impact on both the victim’s and the offender’s self-esteem.[50]
Domestic workload
Another challenge among adolescents that was heightened by COVID-19 is the increase in domestic workload. A study conducted in three states (Bihar, Rajasthan and Uttar Pradesh), showed that 42 percent of 15-24 year-olds experienced an increase in their domestic workload. The pattern has been more clear among adolescent girls (52 percent) than boys (22 percent).[51]
Menstrual hygiene
Access to menstrual hygiene products was neglected during the initial onslaught of COVID-19.[52]Especially during the initial phase of the nationwide lockdown, sanitary napkins were not considered in the list of essential items and there was severe disruption in their production. It was on 29 March 2020 when sanitary napkins were included in the essential list.[53]
According to a survey conducted in 2020 in three states of India,[e]58 percent of girls under 18 years reported an unmet need for sanitary pads.[54]Similar surveys have been conducted in other states,[f]and showed comparable results.[55]The girls who were unable to use sanitary napkins during the pandemic, resorted to unhygienic practices,[56]which could lead to alarming consequences such as toxic shock syndrome, reproductive tract infections (RTI), and vaginal diseases.[57],[58]What compounded the lack of supply was that during the lockdown, the provision of services through Adolescent Friendly Health Clinics (AFHCs) under the National Adolescent Health Programme varied across containment, buffer, beyond buffer, and green zones.[59]
Mental health
Children and adolescents are more vulnerable to mental health issues because they are unable to comprehend the entirety of a situation nor fully communicate their feelings to adults.[60]This vulnerability was heightened as the pandemic disrupted their normal lives, deprived them of schooling and, concomitantly, opportunities for socialisation and physical activities.[61]
As the health crisis unfolded and high amounts of information floated on social media, significant proportions of which were unverified or false—children and adolescents were made even more vulnerable.[62]Many of them suffered anxiety, depression, sleep disturbance, and loss of appetite.[63]
In response to the heightened vulnerabilities of young people’s mental health, the government of India started the programme, ‘Manodarpan’, under which a toll-free helpline number and a website were launched, and a handbook was issued on the life skills necessary to survive a health crisis.[64]Psycho-social support centres, called Snehi, were also set up in different parts of India, where counsellors help children and adolescents navigate the mental challenges wrought by the pandemic.[65]These centres started receiving COVID-19-related calls as early as February.[66]
Some states have conducted their own measures: Kerala, for example, launched the first-of-its-kind student-run helpline, ‘Kutty desk’, as part of a larger programme called ‘Our Responsibility to Children’ (ORC).[67]Over 200 children were selected and trained to run the programme.[68]
Before the pandemic, the government was running the Rashtriya Kishor Swasthya Karyakram (RKSK), launched in 2014 and designed to address adolescent health issues, including mental health.[69]The programme involves community activity and clinic services. However, the pandemic interrupted these community-based activities. In containment areas, teleconsultation was made available to adolescents through AFHCs.[70]
Child labour
Evidence suggests that in times of emergencies and crises, there is higher likelihood of children migrating to cities and entering the labour force.[71] The COVID-19 pandemic threatens India’s commitment to end all forms of child labour under SDG 8, even as the figure has in fact declined by 2.6 million between 2006 and 2011.[72] Compared to adults, children are more likely to take up work for less pay, and be exposed to vulnerable conditions. Indeed, as India began lifting lockdown restrictions, cases of child labour showed a steady rise in June 2020 as compared to the previous months.[73]
Malnutrition
COVID‐19 is certain to impact the food, nutrition, and health security of young children.[74]Data shows that in India, every third child suffers from one form of malnutrition (stunting, underweight, or wasting).[75]According to the Comprehensive National Nutrition Survey (2016-18), 23 percent of children (5-9 years) and 24 percent of adolescents (10-19 years) were thin for their age (BMI-for-age <-2 SD).[76]The current COVID-19 context could aggravate malnutrition among children and adolescents. The nutritional status of children is extremely susceptible to the smallest of shocks to bodyweight. A reduction in child’s body weight between 0.5 and 1 percent can substantially increase the prevalence of underweight and wasting. Estimates say there will be 410,413 and 392,886 additional cases of underweight and wasting, respectively, in India.[77]ALancetarticle on the indirect effects of COVID-19 pandemic in low- and middle-income countries estimated that an increase in wasting prevalence would account for 18–23 percent of additional child deaths per month.[78]
Though there is lack of similar data for children and adolescents in India, a similar situation can be seen in this age group due to the disruption of programmes like the Integrated Child Development Scheme (ICDS) and the mid-day meal programme. The vulnerability would be higher in rural areas as more than half of children rely on these government programmes.[79]Such disruption can only exacerbate food insecurity.[80]
TheGlobal Nutrition Report 2020has taken cognisance of the grave economic crisis due to COVID-19 in developing countries like India.[81]While highlighting the stark inequalities in accessing food and healthcare in India, the report emphasises the underlying importance of maintaining food supply and healthcare systems for the poor while formulating policy responses to COVID-19.[82]
Physical activity
According to a survey conducted with parents of children (5-15 years) in New Delhi, 54 percent said their kids spend an additional average of five hours on a screen every day. A large 84 percent of parents were worried about their child’s increased screen time.[83] Another study conducted among 13-25 year-olds in both rural and urban areas found that average screen time has increased to 5.12 hours from 3.5 hours. The study, however, does not report the age-segregated data for 18 years.[84] As screen time increased, physical activity dwindled. Research has shown that reduced physical activity (and in parallel, heightened sedentary behaviour) are associated with adverse physical and mental health outcomes, such as loss of muscular and cardiorespiratory fitness, weight gain, psychosocial problems,[85] poor academic achievement,[86] and ophthalmic issues.[87],[88] Evidence suggests that the negative impacts may have ripple effects all through to adulthood.[89]
Conclusion
This brief has collated evidence from India that shows how, directly or indirectly, children and adolescents have been severely affected by the COVID-19 pandemic. While these pieces of evidence are still early, it is clear that the impacts are cascading—with one shock building on another, amplifying the direct and indirect secondary impacts that in turn exacerbate instability and leave children and adolescents in a dangerous environment.
To build back better,[90]the imperative is for the Central and State governments, non-government organisations and the private sector to work together in mitigating the severe impacts on India’s young population. Issues like child marriage, mental health, and violence, can be addressed by utilising community-based activities and clinical services under existing national adolescent health programmes.
Studies from India have also recommended that peer educators be used as part of COVID-19-related information dissemination in the community.[91]These trained peer educators are an important link between service providers and adolescents, parents, and the community. They can act as community feedback mechanisms for the various threats facing children and adolescents, and help their peers navigate the manifold ramifications of the pandemic.[92]
This research was undertaken as part of the project, Evaluating the implementation of the Peer Educator Intervention for improving adolescent health in India’s National Adolescent Health Programme. The project is supported by the Medical Research Council (MC_PC_MR/P011446/1).
About the Authors
Deepika Bahl, Shalini Bassi, and Monika Arora all belong to the Public Health Foundation of India (PHFI).
Endnotes
[a]The search engines that were used included PubMed, Google, and Google Scholar. The inclusion criteria were articles and reports published in the English language with children and adolescents as subjects.
[b]DIKSHA is an initiative of the National Council of Educational Research and Training (NCERT) under the Ministry of Education, Government of India.
[c]SDG5: “Achieve gender equality and empower all women and girls.”
[12]India Office of the Registrar General & Census Commissioner, Ministry of Home Affairs, Government of India, “Age Structure And Marital Status”, 2011.
[31]Isabel B. Franco, Paulina Salinas Meruane, and Ellen Derbyshire, “SDG 5 gender equality: not just a women’s issue: sustainable leadership in male dominated industries – the case of the extractive industry”in Actioning the global goals for local impact: towards sustainability science, policy, education, Ed. Isabel B. Franco, Tathagata Chatterji, Ellen Derbyshire, and James Tracey (Springer, Singapore.2019), 69-83.
[51]Population Foundation of India,Impact of COVID–19 on Young People: Rapid Assessment in Three States, May 2020 (Bihar, Rajasthan and Uttar Pradesh),2020.
[57]“Impact of COVID-19 on Young People: Rapid Assessment in Three States May 2020 (Bihar, Rajasthan and Uttar Pradesh, 2020”
[58]Anoop Khanna et al., “Menstrual Practices and Reproductive Problems: A Study of Adolescent Girls in Rajasthan”,Journal of Health Management7, no. 1 (April 2005), https://doi.org/10.1177/097206340400700103.
[70]Ministry Of Health and Family Welfare, Government of India,Guidance Note on Provision of Reproductive, Maternal, Newborn, Child, Adolescent Health Plus Nutrition (RMNCAH+N) Services during & Post COVID-19 Pandemic
[78]Timothy Roberton et al., “Early Estimates of the Indirect Effects of the COVID-19 Pandemic on Maternal and Child Mortality in Low-Income and Middle-Income Countries: A Modelling Study”,The Lancet Global Health8, no. 7 (2020), https://doi.org/10.1016/S2214-109X(20)30229-1.
[79]Sunil Rajpal et al., “Utilization of Integrated Child Development Services in India: Programmatic Insights from National Family Health Survey, 2016”,International Journal of Environmental Research and Public Health17, no. 9 (May 2020), https://doi.org/10.3390/ijerph17093197
[80]Muzna Alvi et al., “Learning in Times of Lockdown: How Covid-19 Is Affecting Education and Food Security in India’,Food Security12, no. 4 (August 2020), https://doi.org/10.1007/s12571-020-01065-4.
[81]Global Nutrition Report,The 2020 Global Nutrition Report in the Context of Covid-19, 2020, https://globalnutritionreport.org/reports/2020-global-nutrition-report/
[82]Global Nutrition Report,The 2020 Global Nutrition Report in the Context of Covid-19
[83]Prachi Verma, “COVID-19 Impact: Screen Time up by 100% for Children”,The Economic Times, June 15 2020, https://economictimes.indiatimes.com/industry/services/education/covid-19-impact-screen-time-up-by-100-for-children/articleshow/76383951.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst.
[84]Shubhajeet Roy et al., “Impact of Covid-19 Pandemic Led Lockdown on the Lifestyle of Adolescents and Young Adults”,MedRxiv,Preprint (2020), https://doi.org/10.1101/2020.08.22.20180000.
[85]Daphne J. Korczak et al., “Children’s Physical Activity and Depression: A Meta-Analysis’,Pediatrics 139,no.4(April 2017), https://doi.org/10.1542/peds.2016-2266.
[86]Eero A. Haapala et al., “Physical Activity and Sedentary Time in Relation to Academic Achievement in Children”,Journal of Science and Medicine in Sport20, no. 6 (June 2017), https://doi.org/10.1016/j.jsams.2016.11.003.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Shalini Bassi is a nutritionist. She holds a Master's degree in Nutrition and Dietetics from the University of Delhi. She has been involved in designing ...
Dr. Monika Arora is a public health scientist working in the area of Non-Communicable Disease Prevention and Control. She is the Director of the Health ...

 PDF Download
PDF Download