Decoding the ban on irrational fixed-dose combination drugs in India
In September this year, the Government of India banned the manufacture, sale and distribution of 328 Fixed-Dose Combination drugs (FDCs) after a protracted legal battle with manufacturers. The ban followed a report by a Supreme Court-mandated experts’ panel that not only was there no therapeutic justification for the ingredients in these drugs, but they can in fact pose health risks. This paper argues that the move against “irrational” and “unsafe” FDCs serves the correct signal to the pharmaceutical ecosystem, paving the way for improvements in the regulatory architecture and patient safety mechanisms. The ban must be viewed not as an obstacle for the pharmaceutical industry, but as a pillar for a stronger Indian healthcare system.
Introduction
The Government of India’s September 2018 decision to ban[1] a sizeable number of “irrational” and “unsafe” Fixed-Dose Combination drugs (FDCs) has been widely seen as a bold decision to prioritise public health and patient safety over the interests of the pharmaceutical industry. With a market worth about INR 16 billion a year,[2] the ban on these drugs will have wider ramifications beyond its immediate impact on the industry’s revenues.
The ban was imposed after ten years of a high-profile legal battle between the Ministry of Health and Family Welfare (MHFW) and activist groups on the one side, and the multinational and domestic pharmaceutical industry on the other.
The banned drugs, 328 in number, include well-known brands that have existed for decades, raising serious concerns about how they were allowed to be sold for public consumption, to begin with. Therefore, it is important for the government and other stakeholders to educate people about the FDCs and their utility, and tighten the country’s drug approval mechanisms. The distinction between ‘rational’ and ‘irrational’ FDCs has to be clear to allow proper space for market realignments to happen and facilitate societal-level improvements that can emerge from a sustained public discourse on this issue.
As witnessed in the failed case of generics taking over branded drugs, in which addition of both generics and branded generics diluted the cause of generics itself,[3]a similar fate may befall this case too, especially considering the presence of a large number of irrational FDCs in the market beyond the number currently under discussion. Some stakeholders either being myopic in their vision or protecting their vested interests may attempt to deny the benefits that the ban would bring. A case in point is the judicial turnaround witnessed over the banning of FDC drugs. Four days after the ban on 12 September 2018, the Supreme Court stayed it for three of the banned drugs. Ironically, all 328 drugs were banned on the basis of the evaluation report of a technical committee mandated by the Supreme Court itself. The committee highlighted grave public health risks posed by these FDCs. The stay in the case of three was granted on the ground that these drugs had been given licence before 1988 and that the committee was not legally allowed to examine or decide on their safety and efficacy.[4]
The pharmaceutical ingredients, or drugs, are basically meticulously processed chemicals, known to have well-researched and documented benefits for human use at certain dosages. For the drugs to be approved for sale, their therapeutic advantage is weighed over their side effects along with proper documentation of the exact quantities of dosage – calculated on the basis of milligram per kilogram body weight – and the frequency of the doses along with total consumption period required for therapeutic effectiveness. Any pharmaceutical company interested in the import or manufacture and sale of drugs within India, by becoming the Marketing Authorisation Holder (MAH) for any new drug or a drug combination, has to first secure the approval of the central regulatory agency, the Central Drug Standard Control Organisation (CDSCO). Further, the MAH is responsible for documenting any adverse effects for four years following the approval of any new licence.
Pharmaceutical ingredients, initially prepared as raw materials called ‘bulk drugs’, are then processed as ‘formulations’ i.e., final pharmaceutical products, which have their intended medical benefits. These formulations are suitably made available for human consumption at a particular dose and are most commonly prescribed as ‘Single-Dose Formulations’ (SDFs). However, for certain ailments – for example, some infectious diseases like tuberculosis and HIV – multiples of such formulations are required to overpower the causative bugs and prevent the development of resistance for the medications. Similarly, some non-infectious ailments such as cardiovascular diseases, diabetes and other chronic diseases are better addressed through a combination of drugs.
In some clinical scenarios that require intake of multiple oral pills and prolonged treatments, there is a margin for non-adherence, partial compliance or intake of wrong dosages; these affect patient outcomes. The FDCs, which are offered as a combination of two or more pharmaceutical ingredients, packed at a certain ratio of doses into a single dosage form, an oral pill – provide an effective alternative to overcome such difficulties. If prescribed correctly, FDCs offer a clear benefit in diseases like malaria, tuberculosis, leprosy and HIV, where drug resistance and larger pill burden are common challenges. In some instances, the cost efficiencies with the combined forms could also weigh in favour of FDCs, when the pharmacological benefit is the same or even better than the same set of drugs taken individually. In those clinical scenarios in which FDCs offer an incremental benefit in their therapeutic effect or convenience or cost, all within the line of safety, it is considered to be “rational” to use FDCs. Such rational FDCs are appropriately recommended for use against specific ailments by the clinical experts of pharmaceutical companies or agencies like the World Health Organization (WHO)[5] and the authorities of disease control programmes, after due diligence on the benefit and having documentation of safety.
FDC Challenge: “Irrational” FDCs, Decades of Neglect
Although having cocktails of drugs in the form of FDCs seems to be advantageous, they are not always beneficial or safe for various scientific reasons. When combined as FDCs, some medications can result in a lessened therapeutic benefit or exhibit a different safety profile, contrary to what could be extrapolated based on the actions of these medicines when used individually. This aspect demands extreme caution from the pharmaceutical companies, careful checks from the regulatory agencies, and due diligence on the part of healthcare providers. Gaps in any of these aspects can result in bringing the ineffective or even harmful FDCs in close reach of patients. Such undesirable combinations, termed ‘irrational’ FDCs, are the real culprits and of serious concern to the patients using them and also pose a larger public health threat to communities. Free availability of a large number of irrational FDCs in the Indian market has been widely discussed and documented over the past decade, even on the international front. The need to weed out these irrational FDCs with urgency and strictly prevent new ones from entering the market is undebatable. Thus, it is important to maintain clear distinction between the rational and irrational FDCs in any discussions on FDCs, which, in India’s case, does not seem to happen with the seriousness it deserves.
Even though the FDCs have been documented in Indian market since the 1960s, efforts to regulate them started in 1988, following a revision of rules under the Drug & Cosmetic Act, 1940. However, one persistent problem has been the gap in having a systematic, transparent and efficient regulatory framework for FDCs in India. The state and central level agencies fell short of full clarity in their roles and mutual confidence in their capabilities while screening and approving new drugs.[6] A disconnected regulatory ecosystem, coupled with an aggressive pharmaceutical industry, gave rise to a challenging domestic pharmaceutical market – one which is flooded with FDCs, including irrational FDCs, offered inappropriately for various ailments and stretched far beyond their therapeutic advantages.
In view of regulation, considering the variability in the effectiveness and safety limits of combination forms, all FDCs fall under the category of ‘new drug’ and therefore needs prior approval of CDSCO after submission of documents showing therapeutic benefit, additional advantage and safety profile. These processes were laid down under Schedule Y, which came into existence in 1988, under the Drug & Cosmetics Act, 1940. As per Rule 122E of the same law, CDSCO as Central Licensing Authority (CLA) approves the FDCs after reviewing relevant pharmacological studies such as bioequivalence, safety profile and documentation related to the initial clinical trials. Only after the approval from CLA for a particular FDC, the state licensing authorities (SLAs) can issue licences for its import, manufacturing, marketing and sales.
However, despite not having adequate technical expertise the SLAs ignored this aspect and ended up directly giving licences for FDCs in numerous instances. Such FDCs would have found their way difficult through the approval process of CLA, whose technically capacity – even though not up to the desired level – is relatively better. Further, MAHs are mandated with post-marketing surveillance and periodic data submission to the CLA for four years after introduction of a new drug. This helps in pooling safety information across larger population groups than what would have been undertaken in clinical trials earlier. Although this aspect has been weak in India – in its implementation in true spirit – it has its own importance for regulatory approvals. Especially since following this four-year period of post-introduction of a new drug, other manufacturers can directly apply for the licence from the SLAs with far less documentation requirements and laxity with regard to pharmacological studies. This literally means that four years after any MAH secures the first-time approval for a FDC, it is an easy ride for other MAHs thereafter. This has given an easy route of entry for several FDCs, especially from the smaller pharmaceutical firms, which lacked capacities to even undertake the relatively less expensive bioequivalence pharmacological studies.
While 1,292 FDCs have been approved officially from 1961 to mid-2018 by the CLA, their actual numbers in the Indian market – including those approved by several SLAs – is estimated to be around 6,000.[7] Further, the total number of brands (for these FDCs) from various pharmaceutical companies runs into tens of thousands. The exact numbers or the systems for accounting of all FDCs are not available. Ironically, in spite of having specific provisions under section 26A of the Drug & Cosmetic Act, CSDCO failed to take prompt action against the large numbers of FDCs that were given direct approvals by the SLAs, which had neither the mandate nor the required technical expertise for this function. Such state-level licences, given over decades, piled up enormously and included those for both rational and irrational combinations, with the latter constituting a much larger fraction. As found by the 59th Parliamentary Standing Committee in mid-2012, even the approval processes for new drugs by the CLA itself had several lacunae, including complacency in complying to its own protocols, lack of transparency and ambiguity in selection of experts and in scrutiny of new drugs.
Deep-rooted factors for explosion of FDCs
The disproportionate growth of FDCs in India, including a large number of irrational FDCs, was fueled by various factors prevalent across the spectrum of the pharmaceutical ecosystem. Precipitating factors include aggressive commercial and at times irrational outlook from the pharmaceutical companies, lapses of regulatory agencies, negligence among medical practitioners and pharmacists and ignorance of both rural and urban public taking non-prescription-based medications either through unqualified practitioners or as self-medication.
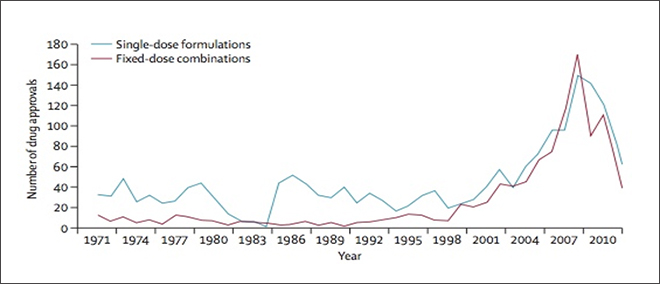
Though the amendments to the Drug and Cosmetics Act, 1940, which happened in 1988 and 2005, introduced some checks, the law has come under criticism for not offering adequate safeguards against undesirable growth of the FDCs. After 2005, consequent to the TRIPS agreement, Indian pharmaceutical companies came under pressure to maintain their growth trajectory. It was during the years 2005-11 that India witnessed a spike in approvals of both SDFs and FDCs by the central regulator.[8] This could be a proxy for what would have unfortunately happened with the state regulators too.
Figure 1. Trends of approvals from CDSCO (1971-2011)
Source: India should introduce a new Drugs Act, January 2014, Lancet
The inclusion of a large number of commonly used drugs under the National List of Essential Medicines (NLEM 2011) and the Drug Price Control Orders (DPCO 2013) also strained the financial comforts of pharmaceutical companies. At the same time, strengthening of the CDSCO and overall regulatory systems that were on the cards for a long time, got significantly delayed in spite of the clear findings and reinforcing recommendations of several government committees and policies. Inordinate delays in the implementation of the recommendations of various committees like the Mashelkar committee for strengthening regulatory framework or the Hathi committee of 1975, which envisioned a stronger national-level drug authority, resulted in a greater leeway for the undesirable pharmaceutical practices to flourish. Pharmaceutical companies also use the route of FDCs to circumvent price reduction mandated for essential drugs – mostly SDFs – under the ambit of Drug Price Control Orders (DPCO), a prominent tool tried by the central government to make drugs affordable. Understandably, pitfalls in the regulatory framework augur well for the shortcut-seeking industry players to maximise profits even when lacking the rationale. This approach – although not unique to pharmaceuticals sector – is detrimental in this case owing to grave public health consequences.
Table 1.Products and Firms most affected of the proposed ban of 344 FDCs in 2016
Categories impacted (in INR Millions)
Big losers (in INR Millions)
Respiratory
13080
Abbott Healthcare
4850
Anti Diabetic
6090
Macleods Pharma
3700
Pain/Analgesics
5560
Pfizer
3680
Anti-infectives
5190
Mankind
2530
Gastro Intestinal
4850
Alkem
1610
Derma
2790
Ipca
1300
Neuro/CNS
490
Medley
1160
Gynaecological
300
Glenmark
1100
Blood Related
30
Franco
1040
Urology
10
Wockhardt
1020
Cardiac
10
Aristo
1020
Source: Revikumar KG, Veena R, Fixed dose combinations in Indian medicine market – a SWOT analysis, MOJ Bioequiv Availab. 2017; 4(3):276‒280. DOI: 10.15406/mojbb.2017.04.00071,
The protracted battle against irrational FDCs started almost a decade ago and passed through significant regulatory, political and judicial processes of security and evaluation. Roots of this battle lie in the central government order of 2007, in which the State Drug Controllers (SDCs) were directed to withdraw 294 FDCs which were licensed without the statutory approval of Drug Controller General of India (DCGI) at CDSCO. Banking on the logic of procedural incorrectness in the Centre’s banning of licences issued by the states, pharmaceutical companies got a stay order from the Madras High Court. The 59th Parliamentary Standing Committee, in its report submitted to Parliament on 8 May 2012, was critical in pointing out to the deficiencies with CDSCO in its role of safeguarding the health of people and provided recommendations to strengthen its functioning.[9] Subsequently in early 2013, the DCGI requested all SDCs to ask the concerned manufacturers to submit their responses within four months and prove the safety and efficacy of their FDCs within 18 months, failing which manufacturing licences would be automatically considered void. More than 6,220 submissions were received from the industry demanding a larger timeframe for their scrutiny. The cumulative approvals given for FDCs by CDSCO from 1961 until then stood far less than a quarter of this number. As a 10-member expert committee was overwhelmed with the task, the Ministry of Health and Family Welfare (MOHFW) constituted a new committee under the chairmanship of Prof CK Kokate in September 2014 to ascertain the rationality of the FDCs. As per this committee’s report,[10] submitted on 10 February 2016, 42 percent of the FDCs were found to be rational as per the available scientific literature, 15 percent were found to be irrational right away and more than 30 percent either needed further careful consideration or additional data. With such a large spectrum of uncertainty over their rationality, 344 FDCs – which were confirmed to be irrational – were banned by the government on 10 March 2016.
With the looming prospect of significant losses, the ban of 344 irrational FDCs was challenged by the pharmaceutical industry through litigations in the high courts of Delhi, Chennai and Bengaluru. The Delhi High Court stayed the ban in 2016. In January 2017, the central government approached the Supreme Court, which had subsequently taken over all the state-level litigations under its purview. The Supreme Court directed the central government to verify all the justifications provided by the industry for the FDCs. The pharmaceutical industry challenged the ban claiming it to be based on recommendations from outside of CDSCO, prompting the Supreme Court to further direct the central government to evaluate the claims through the Drug Technical Advisory Board (DTAB) or its sub-committee. Subsequently, a sub-committee under Dr Nilima Kshirsagar was set up in early 2018. This committee endorsed the earlier recommendations, which helped the government to finally announce the ban. This long and tedious legal process of restricting a fraction of the irrational FDCs in the market highlights the importance of better regulatory mechanisms at the first instance of approval of drug licenses to the MAHs.
Irrational FDCs
Out of the total 433 medicines listed under the 20th edition of the WHO list of essential medicines issued in August 2017, only 37 are FDCs.[11] Similarly, the Indian list of National Essential List of Medicines (NLEM 2015)[12] lists only 24 FDCs out of the total 376. A majority of these FDCs are aimed at improving treatment adherence and preventing drug resistance among the diseases of public health importance such as TB, HIV and Malaria.
Indian domestic market has seen a significant increase in FDCs over the past two decades[13] and with the FDCs itself estimated to be over 6,000, this translates into tens of thousands of product options for clinicians to choose from. While this is certainly not justifiable from the clinical perspective and accepted global norms for FDCs, their predominance among several therapeutic groups and across those with non-prescription related sales and self-medication potential point to the commercial reasons driving this trend.
Another study that tracked the availability and use of FDCs in India over a period of 2007 to 2012 in the therapeutic group of painkillers, scientifically called Non-Steroidal Anti-Inflammatory Drugs (NSAIDS), found that India had 124 FDCs and their 2,739 products of various companies, while in contrast, only six and 10 FDCs were available in the UK and US markets, respectively. These 124 FDCs were contributing to 62 percent of the total oral drug sales of NSAIDS. Of these FDCs, 73 percent did not have CDSCO approval, but were in the market and having 43 percent share among total products available on the shelves.[14]
Table 2. Example of Numbers of FDCs and brands of certain therapeutic groups in India (evaluated in 2011-12)
Therapeutic Groups (use)
FDC related formulations
as of 2012
FDC related Brands
FDC related Sales
FDCs available in India (No.)
FDCs approved by CDSCO % (No.)
FDCs available in UK (No.)
FDCs available in US (No.)
Total brands of these FDCs (No.)
Total Sales of Oral Drugs (in INR crore)
% Sales of FDCs (out of total oral drug sales)
% of FDC sales from unapproved FDC’s (out of total FDC sales)
NSAID (painkillers)
124
27% (30)
6
10
2739
1181
62%
61%
Metformin (for Diabetes)
25
80% (20)
8
10
536
817
56%
99.7%
Antidepressants
16
19% (3)
0
1
301
356
57%
57%
Antipsychotics
10
30% (3)
0
1
211
116
6%
6%
Source: Study across four therapeutic groups in India in 2011-12[15]
Considering the large numbers of drug manufacturers involved in the business of formulations, the list of FDC brands run into thousands under each therapeutic category. It is, therefore, a herculean task for any prescribing doctor or the dispensing pharmacist to remember the various combinations and guide the patient appropriately. As the clinician update-cum-brand promotion activities are primarily driven by the large field force of medical representatives, this in turn, translates into brand-based prescription behaviour of clinicians, creating a difficult scenario for promotion of generics too. This is the predominant trend for drug sales, where the irrational FDCs comfortably pass through the sales counters. Non-prescription-based sales by the pharmacists and opportunity for replacement of the brands at the retail pharmacy level are other contributing factors for promotion and rampant growth of FDCs.
Another important aspect of the irrational FDCs is driving Antimicrobial Resistance (AMR) when at least one of the medications is targeted against micro organisms. The irrational FDCs with sub-standard doses of antimicrobials, which fail to offer adequate therapeutic response to successfully kill the bugs, would end up rather helping them develop resistance to the FDCs. Over a period of time, the bugs gain capabilities to survive against even the correct regimens as well as rational FDCs. Analysing the sales data for antimicrobials in India between 2011 and 2012, researchers from the Queen Mary University, London, found that out of 118 FDCs involving antimicrobials, only 36 percent had CDSCO approval and could be assessed for their rationality as per the Indian standards.[16] Further, of these 118 FDCs only 3.4 percent were found to be approved in the US and UK markets.
Doses of individual medicines in certain fixed ratio demand the choice and use of FDCs only by experienced clinicians and trained pharmacists who understand their effects. Paradoxically, however, unqualified medical practitioners take maximum advantage, considering FDCs as the ‘all-in-one’ convenient option for their practice of quackery. While such large numbers of FDCs are bound to cause confusion among the healthcare providers and promote nonprescription sales though pharmacies and quacks, irrational FDCs add greater challenges, such as toxicities and antimicrobial resistance. As a consequence, both the high number of FDCs and a much higher proportion of unapproved or irrational FDCs can be catastrophic, considering the adverse clinical outcomes and the economic burden in managing the consequences of these outcomes.
Improving regulatory systems in India
FDCs: Broader Concerns in India’s Health System
Although FDCs offer cost savings across the pharmaceutical supply chain – right from production and packing to transportation and marketing – they can never outweigh the scientific rationale in the critical life-saving and heavily regulated pharmaceutical industry. The elaborate process – including legal hurdles – that the recent announcement to ban the irrational FDCs had to overcome has exposed the glaring lacuna in both the regulatory and health systems in India.
Regulatory and other government agencies, both at the state and centre, have failed to curb the entry of unnecessarily large numbers of FDCs and irrational FDCs into the market. Their use is documented even among the tertiary care hospitals across the country.[17][18] While the lack of clarity on the role and coordination between the state and central agencies have compounded the problem,[19] regulatory agencies at both the levels continue to suffer from inadequate in-house expertise, hampering their capabilities of due diligence in handling new drug applications. Coordination between the medical fraternity and pharma regulatory officials has neither been strong nor broad enough to evaluate and match the clinical or healthcare needs in the country with the ambitions and strengths of the domestic pharmaceutical industry.
Slack enforcement actions on large numbers of unqualified medical practitioners and failure in controlling non-prescription-based sales continue to haunt the healthcare ecosystem in many ways. One of the interlinked problems is the disturbingly large numbers of FDCs through their brands in the Indian market. Marketing practices of drug companies influence the prescription of brands by the private health care practitioners, who cater to over 70 percent of the outpatient consultations where the scope for FDCs is high. This has repeatedly come under public scrutiny. However, except for partial success in restricting pharmaceutical companies from actively sponsoring medical practitioners and attempts of the central government to popularise generics, the government agencies, health ministry and professional councils are yet to come up with dependable and workable mechanisms to rectify these anomalies around dependency on brands. Drug companies continue to rampantly promote brand-based sales of both rational as well as irrational FDCs with aggressive marketing strategies. Medical practitioners currently do not have any alternative and credible platforms – from the professional associations or government agencies – to remain updated on the rational drug innovations and combinations but are forced to choose from an unnecessarily large number of brands being made available in the market.
The medical fraternity and leadership of the medical associations primarily remain narrowly focused on the immediate issues around their practice, leaving the difficult tasks of advocacy, debate and litigation efforts against the mighty drug industry to the smaller stakeholders such as health activists and NGOs. Except for advocacy by a small fraction of medical professional bodies, such as the Indian Association of Dermatologists, Venerologists and Leprologists (IADVL),[20] the efforts of major medical professionals’ associations are hardly visible. Proactive and concerted efforts by both private and public healthcare providers and professional forums to restrict the unnecessary and irrational practices are lacking at the points of prescription i.e., at the clinics, as well as at the point of dispensing the medicines i.e., pharmacies. Such slackness among the health sector champions offered unrestricted freedom to several undesirable drug marketing strategies aiming to maximise profit margins, even at the expense of rationality and safety. Irrational FDC is just one, though an important one, among a set of challenges facing the health sector.
In recent years, an increasing political commitment for health – both at the central and state levels – is driving various policy reforms for greater public good. Pharmaceutical policy reforms, price control for drugs and medical devices, efforts to regulate clinical establishments and revisions in national policies for healthcare are some notable examples. These measures are aiding the refinement of debates and deliberations on public health and universal healthcare among the stakeholders across the verticals of healthcare, pharmaceuticals, insurance and finance.
More specifically, the involvement of various stakeholders through government-constituted committees and subcommittees to deliberate on the issue of banning irrational FDCs is a good sign. Efforts to strengthen the regulatory mechanisms under CDSCO with significant financial commitments allocated under the 12th five-year plan, although started late, need to be sustained until significant overhaul of the pharmaceutical as well as the overall healthcare sector happens as envisioned in the national policies and as recommended by various committees, including the 59thParliamentary committee. Bringing a logical conclusion to the issues surrounding irrational FDCs – which started to tarnish the image of Indian pharmaceutical system on the international front – gives confidence to the civil society and even the drug industry on the regulatory scenario and democratic processes. Such combined efforts of both government agencies and civil society against the undesirable practices of the mighty Indian pharmaceutical industry will assure public health stakeholders on government’s priority to safeguard broader public health interests over the industry growth requirements.
Foremost among the tasks of the Government of India – in the best interests of people and the pharma industry – is to adopt a strict policy of non-tolerance against irrational FDCs. Any dilution in the ongoing momentum of regulatory improvements, implementation of corrective actions or interpretation of the legal stance towards restricting the large numbers of irrational FDCs from reaching the public, will lead to a far more complex scenario in the future. Any slackness in resolving the problem of irrational FDCs can result in a further drain on time and resources while continuing to jeopardise clinical outcomes and health budgets.
In view of the looming public health threat from the irrational FDCs, government needs to consider the following steps, as part of a time-bound exercise to comprehensively resolve the problem:
Reference scientific documents and standards, which form the basis of rationality for FDCs, need to be publicised immediately and regularly updated. National formulary – i.e., the reference list of prescribable drugs – should be updated accordingly.
Sets of conditions, which are currently used for the manufacturing and marketing of FDCs but are not justifiable, need to be released for self-evaluation and initiation of steps for their voluntary withdrawal by the MAHs. This can also serve as a guide for healthcare providers, both physicians and pharmacists, to evaluate their use at their respective levels.
Instead of the current, excessively time-consuming approach of evaluating rationality of FDCs on an individual basis, a simpler and legally tenable broad framework – to evaluate thousands of FDCs on their rationality and the need for their market presence – should be developed by the MOHFW after duly seeking inputs from the industry, civil society and professional and legal experts.
Building on the recent and the ongoing experiences – from the elaborative exercises of evaluating larger numbers of FDCs to the banning of irrational FDCs – a foolproof screening criterion should be formulated for the approvals of rational FDCs in the future. This should allow to clearly fix accountability for and promptly red-flag the erring actions of officials at the levels of CLA and SLA, who give the approvals, or any MAH, who seeks fresh approvals or continue to market irrational FDCs.
A dedicated online portal displaying the comprehensive list of rational FDCs and the list of FDCs approved with all their respective brands should be facilitated by government to help all stakeholders to promote only the rational FDCs. Such a portal should also list all the irrational FDCs that are being removed from the market.
The current exercise of weeding out 328 irrational FDCs from the Indian domestic market will not and should not be an isolated event. Rather, it has the potential to lay the foundation for a series of long-lasting improvements for the pharmaceutical and healthcare delivery sectors, for which further stakeholder-specific recommendations are listed below.
Pharmaceutical industry
Drug companies, irrespective of their size, especially those having products that feature in the banned list of irrational FDCs, need to build their sales strategies strictly on rationality rather than on marketing tricks. It should be inferred that maturing regulatory scenario in India, which is embracing harmonisation on the international front, will offer room for products, processes or approaches only on the basis of rationality in the future.
Considering that some of the oldest and most popular household brands from the multinational pharmaceutical giants have faced ban or are being questioned, drug companies must realise that political lobbying for irrational practices will be less successful hereafter, with the improving governance ecosystem and increasing public activism.
Considering the large number of FDCs still in the market, the drugs industry, led by pharmaceutical associations, should take the lead in rationalising their product portfolios and even consider facilitating voluntary withdrawal of irrational FDCs from the Indian market and those meant for export markets.
In the light of increasing public awareness about safety, drug companies or brands – irrespective of their size and brand value – risk regulatory backlash and loss of customer confidence, which will be costlier to rebuild. While the recent action of the government offered enough time for companies to mitigate the impact of the ban, it might not be the same case in the future. Hence, marketing budget allocations, large-scale investments via mergers and acquisitions of companies or brands have to factor in the rationality of products while accounting for their financial credentials.
Pharmacists/Retail chemists
Several ongoing developments in healthcare delivery – right from the need for prescription audits under accreditation requirements to the need for identifying irrational FDCs at the point of medical care – offer a prominent role for pharmacists in the healthcare delivery sector, in addition to their traditional roles in retailing or in manufacturing.
The changing profile of demographics and diseases, including the increasing burden of non-communicable diseases, broadens the need and scope for pharmacist-based guidance and counselling during various stages in the course of disease management. The concept of ‘community pharmacist’ – picking up in many countries but unheard of in India – needs to be embraced to address the transitioning health status of communities and help in screening the rational versus irrational FDCs.
Medical practitioners – mostly hard-pressed for time – need to be supported by pharmacists in briefing and cautioning the clinicians on the efficacy or safety issues of medical formulations, including FDCs.
Regulatory and other government agencies
A comprehensive list of all FDCs in the Indian market along with the details of rationality will help clinicians and pharmacists in using them with discretion. Regulatory agencies should establish a mechanism to account for all FDCs, and their linked brands and publicly display the details with periodic updates of the opinions and final reviews from any of the government technical committees, regulatory agencies of developed nations and other professional bodies identified by the government.
The MOHFW should undertake measures to ensure and strengthen seamlessness in the roles and responsibilities of agencies across the centre and the states.
Instead of ad-hoc committees, CDSCO should have a diverse pool of clinical experts transparently selected from across the country and made available for government with fixed term arrangement or deputation for at least three years or for five years, if coming on board while retaining their other roles.
In spite of the discretionary role of the centre in approval of new drugs, including FDCs, the subject matter experts and expert committees available at the central level should be shared and made available for the state-level needs.
States should be encouraged and supported to have their own technical committees and expert panels to submit their concerns and seek actionable insights on pharmaceutical issues, including FDC-related issues, considering the state-specific health challenges, disease outbreaks and patient demographics. Inclusion of representation from the states in national-level committees and supranational forums can help government build a robust and cost-efficient network of expertise for a large country like India.
Pharmacovigilance Programme of India (PvPI) started in 2010 has grown several folds with an increasing number of Adverse Event Monitoring Centers (AMCs), mainly anchoring around major teaching institutions which are also multidisciplinary knowledge hubs. Such centres, as they get stabilised, can be optimally utilised for conducting education and awareness programmes on FDCs along with periodic screening of FDCs in alignment with latest scientific evidence.
To strengthen the accountability of the MAHs, the post-marketing surveillance period, currently for four years, should be made extendable based on the analysis of initial evidence. Strict penalties must be considered for the MAHs who continue to sell FDCs even after emergence of scientific literature contrary to the earlier findings based on which the approval was given.
Uniform Code of Pharmaceutical Marketing Practices (UCPMP), a progressive step introduced in 2015, has been left for voluntary adoption by the pharma industry. This measure was initially introduced only for a period of six months, but the government has been passively continuing its role. The UCPMP, still in place on voluntary adaptation basis, is set to become mandatory with the draft order, “Essential Commodities (Control of Unethical Practices in Marketing of Drugs) Order, 2017” awaiting its final approval. This legislation needs to be finalised soon to help enforcement agencies to keep a check on the irrational marketing and promotional practices of the pharmaceutical products.
The ongoing processes of literature monitoring and post-marketing surveillance, which are primarily based on fulfillment of the compliance requirements of MAH, needs to be reviewed to capture and document only true experiences of the end-users. If found necessary, the norms for submissions of Individual Case Safety Reports and Periodic Product Safety Updates can be kept flexible and more realistic to collect the data proportional to the ongoing marketing of pharma companies and the consumption patterns of the FDC brands. Random cross-verifications of small samples of these submissions can be institutionalised with linkages through the AMCs.
CDSCO and MOHFW should continue to improve coordination with regulatory agencies of other countries to ensure mechanisms for cross-reference and prompt rectifications. India’s efforts to strengthen its wider collaboration through the International Conference of Harmonisation and other international platforms including WHO can include the aspect of FDCs as well to help strengthen the vigilance channels of agencies involved in licensing and enforcement.
MOHFW should formulate and periodically update reference lab testing standards for all FDCs getting approvals and made available in the market, with the cooperation of WHO, supranational reference labs and other regulatory agencies of developed nations.
Government must consider investing on public awareness initiatives in partnership with NGOs, teaching institutions and civil society representatives by including FDCs as a sub-component of a broader communication agenda on drug safety and health literacy. Both the centre and states should engage professional institutions for public education and optimise operations of various government initiatives such as promotion for generics, PvPI, consumer engagement initiatives with inclusion of concepts around FDCs.
General public, civil society and patients
Self-medication and over-the-counter sales of prescription medications being widely prevalent in India, responsibility of rationally seeking medications should be built into the public conscience through behaviour change communication campaigns spread across the channels available with the pharma companies, health facilities, retail shops and civic awareness initiatives.
As part of a public education campaigns which are customised at regional and state levels, public needs to be informed about the basic pharma concepts, appropriate practices and safe use of medications, while empowering them with convenient access to the network of centers offering authentic information and quality assurance. Opportunities through Drug Information Centers (DICs), AMCs or the National Health Information Portal should be explored for making information available, customised ailment wise, including the scope for FDCs.
Public should be motivated to avoid self-medication behaviour or directly seeking medicines from pharmacists. Civil society activists and NGOs should broaden their networks by partnering with medical professionals, professional associations and patient associations along with proactive involvement in the government schemes for monitoring adverse events.
Medical Practitioners
Medical practitioners should get sensitised and knowledgeable about various concerns in the pharma sector, including the issues around FDCs. They should evolve with programmes, which are in fact custom-tailored to their specialty of medical practice and strengthen their role in pharmacovigilance activities – complementing the activities of MAHs in recording and reporting adverse events.
Professional associations of medical practitioners should play a leadership role in addressing the pharmaceutical issues ailing healthcare system, including FDCs and work towards rationalisation of prescription behaviours, antibiotic stewardship and rational drug use promoting patient safety.
Medical fraternity, through their associations, should establish collaborative platforms for the regulatory agencies and the Indian Pharmacopoeia Commission and get simultaneously involved in the processes of finalisation of drug formularies and periodic evaluation of the rationality of pharmaceutical products, instead of sharing their expertise and time mainly on an ad-hoc basis as is the case currently.
Conclusion
As stated in the National Health Policy 2017, the Government of India aims to attain the highest possible level of health and well-being for all by shaping effective health systems in all its dimensions. While various actions of the central government – such as price control on drugs and medical devices and the ambitious rollout of Ayushman Bharat – are all set towards the realisation of these objective, the government must also sort out the concerns in the domain of pharmaceuticals. The recent episode of irrational FDCs highlights a serious concern. The struggle that the government has had to face on irrational medicines is enormous, especially when these drugs should have not been in the market in the first place. Since FDCs contribute more than 50 percent of the domestic pharmaceutical market (estimated to be over INR 1,000 billion), concerns around irrational FDCs and their large numbers are pertinent, deserving of firm resolve from the government.
Various studies show that the presence of irrational FDCs across India – even among the tertiary care hospitals and widely used across multiple therapeutic groups – contribute to poor patient outcomes. As documented by collaborative research teams from the UK and India, the presence of 124 FDCs and 2,739 brands in the Indian market in 2011-2012 for painkillers, with only 30 percent having the approval of the CDSCO, highlights the scale of the problem in one of the most commonly used therapeutic segment. In contrast, only six FDCs and 10 FDCs were approved in well-regulated markets of the UK and US, respectively. Beyond the impact of poor clinical outcomes from irrational FDCs, it is a much larger public health concern, especially with the irrational FDCs containing anti-microbial agents. Of the 118 such FDCs that are found in the Indian market by the researchers, only 36 percent had approval from CDSCO. In comparison, only 3.4 percent had approvals in the US and UK.
The root causes for the explosion of FDCs in India, amidst the aggressive marketing strategies of pharmaceutical companies, lie in the decades-old shortcomings of the country’s regulatory framework both at the state and central levels. States issuing approvals directly and bypassing the central authority has led to the availability of more than 6,000 FDCs in the market against the 1,292 official approvals given by the Centre since 1961. As pointed out in the 59th Parliamentary Standing Committee report, even some practices at the CDSCO reflected disregard for patient safety while prioritising the interests of the pharmaceutical industry.
Though the Government of India initiated steps to restrict the availability of FDCs approved by the states in violation with the rules under the Drug and Cosmetic Act in late 2007, it actually resulted in a 10-year-long exercise including legal battles, which ultimately culminated with directions from the Supreme Court for the government to ban 328 irrational FDCs. While the pharmaceutical industry continues to fight the ban— and has succeeded in getting a stay on the ban on three of those FDCs—there is a larger number in the market that needs to be examined. It is important to ensure that the corrective course of action on irrational FDCs does not get derailed and a logical long-term solution is set into motion to prevent both unnecessarily large numbers of FDCs and the irrational FDCs for the future.
Syncing with all other ongoing improvements in health sector, only effective collaboration of all stakeholders can significantly help the nation progress towards a dependable, equitable and rational healthcare system. This will be possible only when the pharmaceutical companies, physicians and pharmacists take cognisance of the problem and work towards the larger public health interests. The 537-page Gazette Notification dated 8 September 2018 that enforced the ban on 328 irrational FDCs should be viewed as an important building block in India’s healthcare and not as an obstacle for the drug industry.
[3] Historically, branded drug is generally a product of innovator company who has undertaken expensive clinical trials or its authorisation holder who markets the drug under a brand name, fixing the price inclusive of all R&D costs, royalty payments and marketing costs. In 1980s, with a view to bring down price of medicines, the US government started issuing manufacturing and sale licenses for innovator drugs post- expiry of the patent protection period to other companies too, depending on the less expensive bioequivalence studies. Such drugs, marketed with their chemical names are called generic drugs and come at a significantly lower cost. When the same concept came to India, established pharma companies selling branded drugs also started their own versions of generics as branded generics, pricing their products in between the ranges of branded and generic drugs. This resulted in a complex and confusing scenario for the generic drug market in India, in which the cost saving benefits of generics could not be ensured.
[6] Roderick Peter, Mahajan Rishikesh, McGettigan Patricia and Pollock Allyson M, “India should introduce a new Drugs Act”, 18 January 2014, The Lancet, (accessed September 17, 2018).
[8] Roderick Peter, Mahajan Rishikesh, McGettigan Patricia and Pollock Allyson M, “India should introduce a new Drugs Act”, 18 January 2014, The Lancet. (accessed September 17, 2018).
[19] Roderick Peter, Mahajan Rishikesh, McGettigan Patricia and Pollock Allyson M, “India should introduce a new Drugs Act”, 18 January 2014, The Lancet. (accessed September 17, 2018).
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

 PDF Download
PDF Download