-
CENTRES
Progammes & Centres
Location
 PDF Download
PDF Download 
Md Kamruzzaman, “Climate Change and Healthcare in the BIMSTEC Countries: Potential for Cooperation”, ORF Issue Brief No. 300, July 2019, Observer Research Foundation.
The countries of the Bay of Bengal Initiative for Multi-Sectoral Technical and Economic Cooperation (BIMSTEC) are particularly susceptible to the adverse impacts of climate change due to myriad factors including large coastal areas, densely populated coastlines, and reliance on agriculture.[i] Indeed, global warming has implications for the public health of the region’s staggering population totalling nearly 1.75 billion.
The impact of climate change on human health can be severe (See Figure 1). Phenomena like rising temperatures, erratic rainfall, and severe floods are associated with diarrhoeal and other vector-borne diseases including malaria and dengue.[ii] Despite these immense threats to public health, climate change could also potentially provide a significant global health opportunity.[iii] The adverse impacts of climate change necessitate that global health responses adopted by nations across the world be adaptive, responsive, and sustainable. Given the similarities in their contexts, BIMSTEC countries require a collective regional approach to mitigate climate-related health risks.
Figure 1: Pathways to potential health impacts of climate change
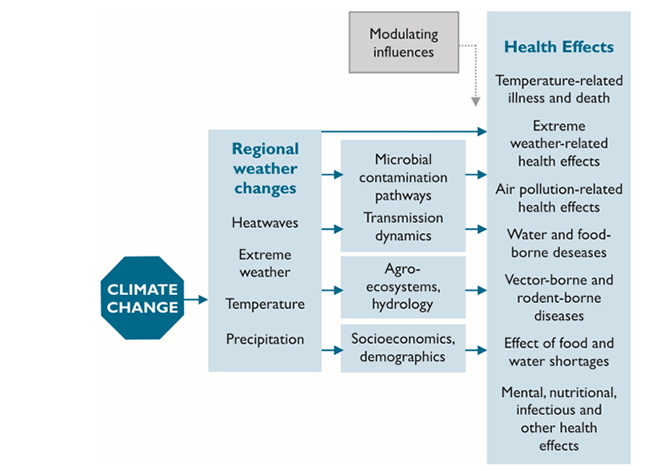
Source: Adapted from WHO (2003)[iv]
This brief identifies common financial and climate change-related public health challenges currently threatening these countries, and inquires into the status of integration of climate change and health into their national-level policies. The brief identifies five multifaceted and collaborative regional agendas that require urgent implementation to provide respite from the health risks associated with climate change.
BIMSTEC countries face similar public health risks from climate change. Due to changing climates, people in Bangladesh, Bhutan, India, Nepal, and Sri Lanka are expected to experience mortality and morbidity due to vector and waterborne diseases such as diarrhoea, cholera, malaria, and chikungunya.[v] Moreover, there is substantial evidence regarding the adverse impacts of rising temperatures in South Asia. For example, the 2015 heat waves across India and Pakistan claimed over 3,000 lives in both countries.[vi] The effects of temperature rise are disproportionate across social hierarchies. A study shows that the incidence of heat-stroke among rickshaw-pullers and industry workers has increased more recently.[vii]
Along with vector-borne diseases, climate change will also affect nutritional outcomes by magnifying food insecurity. Carbon dioxide concentration is likely to reduce the nutritional content of crops such as rice, wheat, and barley, which are staple foods in the region.[viii] A staggering 5 to 170 million South Asian people are predicted to become malnourished following a 5 to 30 percent fall in crop production by 2050.[ix]
Historically, in response to localised food scarcity and associated austerity, people have been forced to migrate to regions with better food accessibility.[x] Forced displacement also arises due to urgent health concerns and loss of habitable land and livelihoods.[xi] South Asia has previously, and continues to experience climate-induced transboundary migration.[xii] Moreover, disease outbreaks are common among displaced populations,[xiii] posing health risks for host communities. In this regard, it is critical that BIMSTEC countries pay adequate attention to climate-proofing different sectors of the economy, particularly health, to avert future crises.
In 2017, Sri Lanka, Nepal, Bangladesh, and Thailand were among the 10 countries most affected by climate change. Growing public health risks impose huge monetary costs on countries, and yet, national spending on healthcare in the BIMSTEC region is miserably low (See Table 1). This has major implications for the region’s vast population — especially the poor — who are at the risk of being pushed down the poverty line without a proper safety net in place to protect them.
Most countries spend less than two percent of their GDP on health. Bangladesh fares worst among its neighbours at 0.4 percent of GDP over a 20-year period, followed by India, whose expenditure was also below one percent in the same period. Due to lack of public expenditure, people resort to out-of-pocket spending for healthcare services. Except for Thailand and Bhutan, citizens in the BIMSTEC member countries have had to spend more than 50 percent, and in many cases as high as 74 percent, to finance their health needs. Evidence shows that environmental factors like climate change worsen a household’s burden of out-of-pocket expenditure.[xiv] In other words, catastrophic healthcare expenditure associated with climate change is likely to further marginalise impoverished and vulnerable communities since they lack physical and financial access to healthcare systems.
Table 1: Climate risk and budgetary allocations for the health sector in the BIMSTEC region
| Country | Climate Risk Index Rank (2017) a | National health expenditure (% of GDP)b | Share of Out-of-pocket expenditure in total health expenditure (%) c |
| Sri Lanka | 2 | 1.7 | 50.1 |
| Nepal | 4 | 1.2 | 55.4 |
| Bangladesh | 9 | 0.4 | 71.9 |
| Thailand | 10 | 2.9 | 12.1 |
| India | 14 | 0.9 | 64.6 |
| Myanmar | 69 | 1.0 | 74.0 |
| Bhutan | 124 | 2.6 | 20.1 |
Note: a= Ranking according to the climate risk index 2017
b= Average annual share of GDP based on 20 years (1998-2017)
c= World Bank data for 2016
Source: World Bank;[xv] Eckstein, Künzel, and Schäfer[xvi]
Among its 14 priorities, BIMSTEC has identified public health and climate change as crucial areas for cooperation. While previous cooperation efforts in public health were along the lines of traditional medicine, the launch of the JIPMER-BIMSTEC Telemedicine Network in July 2017 demonstrates the platform’s growing emphasis on modern medicines and technology, sharing of knowledge, and strengthening links between medical institutions within the region.[xvii] Moreover, in the Fourth BIMSTEC Summit Declaration in 2018, member countries agreed to address non-communicable diseases and other regional public health issues that threaten to undermine the prosperity of the region.[xviii] They also agreed to establish an Inter-Governmental Expert Group to develop a plan of action for fighting climate change and increasing preparedness for disaster management in the region.
Indeed, most countries in the region are still developing a climate change national action plan. Moreover, there has been negligible or no integration of climate change into these countries’ respective health policies.[xix] Lack of such policies will heavily undermine present and future cooperation efforts in the BIMSTEC region’s public health arena.
The following sections provide a brief overview of state of integration of health and climate change in national policies in the BIMSTEC countries.[xx]
The country established the Climate Change and Health Promotion Unit under its Ministry of Health and Family Welfare (MoHFW). Since 2015, the second National Action Plan is being developed. Health adaptation and mitigation strategies are reflected in the climate change action plan. Although these strategies have been given priority, climate change has yet to be integrated into the health policies. Recently, several activities such as community-led adaptation, research on climate change and health, and edutainment campaigns have been implemented.
Bhutan has yet to adopt a health and climate change policy. The country formally initiated the development of the Health National Adaptation Plan in 2016. Climate change related policies are coordinated through the National Adaptation Programme of Action (NAPA) and Second National Communication (SNC). The former covers some aspects of health and health-related vulnerabilities while the SNC covers health as a “standalone and a cross-cutting issue”. Moreover, the health sector prioritises water and sanitation engineering, diseases related to malaria, dengue, Japanese encephalitis, and emergent diseases such as kala-azar (Visceral leishmaniasis), chikungunya, filariasis and diarrhoeal diseases, malnutrition, food insecurity, and respiratory diseases.
In 2008, the Prime Minister’s Council for Climate Change drafted the National Action Plan on Climate Change. The initial draft articulated various climate-related missions, including ‘Sustaining the Himalayan Ecosystem’ and ‘Green India’. Even though health did not receive a priority mission status in the draft, proposed programmes had provisions for the assessment of disease burden owing to climate change and the improvement of healthcare services.
Almost a decade later, in 2016, India’s MoHFW drafted the first National Action Plan on Climate Change and Health. The plan has six broad objectives:
Myanmar drafted the Myanmar Climate Change Strategy & Action Plan (MCCSAP) 2017-2030 which provides a 15-year roadmap to steer Myanmar’s efforts towards addressing climate-related risks.[xxi] Through a holistic approach, the plan aims to develop a pathway to achieve climate resiliency and promote low carbon development initiatives.[xxii] MCCSAP also identifies an implementation framework for the coordination and implementation of such activities. The strategic plan has identified six key sector entry points to achieve its objectives among which one has been directed towards health and wellbeing:
Nepal — like Bhutan — has a NAPA, which was enacted in 2010 and identifies public health as highly sensitive to climate change. Over the years, the country has launched multiple climate change-related policy documents that prioritise public health as one of the sectors most vulnerable to climate change.
In addition to the NAPA report, several policy documents have been launched, including the Climate Change Policy 2011; the Nepal Health Sector Programme – Implementation Plan II (NHSP-IP 2) 2010–2015; the National Health Policy 2014; the National Health Sector Strategy 2015– 2020 and its implementation plan (2016–2021); and the Health National Adaptation Plan (H-NAP): climate change and health strategy and action plan (2016–2020). In addition to other activities, the H-NAP has the following objectives:
Over the years, Sri Lanka has emphasised the importance of climate change through the development of policy documents. In term of implementation, the country has undertaken assessments of climate change impacts, vulnerability and adaptation for health.[xxiii] Sri Lanka has prepared the National Adaptation Plan for Climate Change Impacts 2016-2025. The document has identified health as one of the sectors most vulnerable to climate change.[xxiv] Four key areas have been identified under health, including climate-altering pollutants, spread and outbreaks of diseases, health impacts due to hazardous events, and heat/thermal stress.[xxv] To combat these issues, the following activities have been suggested:
Thailand does not have an official health adaptation strategy yet. Currently, the National Climate Change Master Plan (2013-2015), the 2015-2020 Health Strategic Plan on climate change and health, and the Health National Action Plan are in queue to be adopted at the national policy level. Meanwhile, Thailand has established a climate change and management division as the national focal point. The country has also pursued activities on health adaptation and enhancing institutional and technical capacities related to climate change. National assessments of climate change impacts, vulnerability, and adaptation for health have also been conducted.[xxvi] However, the country has yet to develop an integrated Disease Surveillance and Response (IDSR) system.
In view of the looming threat of climate change and the associated health impacts, it is imperative that the BIMSTEC countries commit to faithful regional cooperation. Due to the existing diversity in capacity and comparative advantages among the BIMSTEC members, effective cooperation has the potential to yield immense benefits for the whole region and beyond. Despite such possibilities, these countries have previously lacked the necessary enthusiasm to consolidate their efforts towards fighting climate change. Against this backdrop, climate-related health challenges need to be incorporated in any proposed vision statement. The following transformative and innovative recommendations are suggested to revamp the efforts of BIMSTEC for stronger regional cooperation:
The joint statement of the Fourth BIMSTEC Summit underscored the need for “defining a long-term vision and priorities for cooperation”. Incorporation of climate-related health challenges in the vision statement will provide the BIMSTEC platform the necessary guidelines for long-term action and reinforce its commitment to fighting climate change and public health risks.
After 20 years, the BIMSTEC Free Trade Agreement (FTA) has yet to see the light of day. There is empirical evidence that the FTA has potential economic benefits for the region.[xxvii] Additionally, trade agreements can enable countries to achieve climate goals by “removing tariffs and harmonising standards on environmental goods and services, and eliminating distortionary and poorly designed subsidies on fossil fuels and agriculture”.[xxviii] Thus, the BIMSTEC members need to work to implement a climate-friendly FTA. A conceptual understanding of the risks associated with climate change will facilitate the process. To enhance this understanding, it is necessary to adopt a bottom-up approach of production and sharing of knowledge involving community-based organisations.
The platform should be committed to sharing good practices in confronting climate change and addressing health risks through the participation of multiple stakeholders including government, development partners, civil society, non-government organisations, academia, and the private sector from the BIMSTEC region and beyond. In addition, the platform should prioritise the participation of local agencies that collaborate with grassroots stakeholders in developing and implementing community-based climate adaptation actions.
Under the flagship of BIMSTEC, a committee should be established to oversee the platform’s operation and activities. The committee members should include members from leading NGOs and community organisations with a proven record of activities in the arena of health and climate change across the BIMSTEC region. In addition, membership should be open for development organisations and civil society organisations that augment advocacy and action for climate change. Lessons learnt through the platform should be harnessed towards strengthening the policy-making process.
Health adaptation to climate change will require significant financial resources. As identified earlier, the majority of the BIMSTEC members are unable to allocate a satisfactory amount of financial resources towards their health sectors. In that regard, through a legal framework, a regional trust fund should be established to provide the members with ample financial resources for undertaking health adaptations.
The fund should be geared towards the facilitation of three major actors across the region: governments, the private sector, and NGOs. First, government bodies from member countries should be able to utilise this fund through grants or soft loans to finance their health sectors. Second, a portion of the fund should be allocated to regional academic and healthcare institutions to encourage research on health risks, training of physicians, and developing curricula for medical education. Lastly, the trust fund should also finance activities of NGOs and community organisations dedicated to building awareness and resilience, and enhancing community-based adaptation to health and climate change-related vulnerabilities.
Along with BIMSTEC member countries, the private sector should also be leveraged to contribute to the fund. More importantly, effective monitoring, accountability and transparency will be necessary to ensure the effective utilisation of the fund.
BIMSTEC member countries need to take the initiative to resolve ongoing regional disputes. Currently, the ambitious cooperation efforts in the BIMSTEC region are threatened by regional disputes and complications of three members – Bangladesh, India, and Myanmar. Current and future cooperation efforts in the region are at the risk of being undermined by the unresolved Teesta water-sharing problem between India and Bangladesh, and the continuing Rohingya refugee crisis. As Bangladesh is at the centre of both complexities, the country’s bilateral ties with India and Myanmar could be stalled.
The Teesta basin is already severely impacted by climate change, as evidenced by recent erratic rainfall and extended hot and dry days.[xxix] As the situation worsens and competition for scarce water resources increases over time, the political and social stability of the region is being threatened, with upsetting consequences for regional cooperation efforts.
Furthermore, Bangladesh is currently hosting over a million Rohingya refugees from Myanmar. Unless the affected population is repatriated soon, US$17 billion will be required for a ten-year period.[xxx] This cost, however, does not include the environmental costs emerging from the crisis, which means the monetary burden is likely to be even higher. In the face of declining foreign assistance, the financial burden of hosting the refugees will fall upon the government of Bangladesh, which is already struggling to finance its development activities. Without regional support from neighbours, it will be nearly impossible to find a resolution to the crisis.
The latest BIMSTEC summit was silent on the Rohingya issue, which is a cause for concern. As a platform to promote regional development and connectivity, the BIMSTEC initiative needs to assist these countries in resolving the crisis. Otherwise, worsening diplomatic ties between Myanmar and Bangladesh might stall the BIMSTEC process. Consequently, the platform might suffer the same fate as its predecessor —the South Asian Association for Regional Cooperation. Therefore, it is imperative that the BIMSTEC platform plays a proactive role by facilitating energetic diplomacy to reach a solution.
Both climate change and public health have been clearly delineated in the 14 areas of regional cooperation among BIMSTEC member nations and must be addressed to achieve sustainable development. This brief highlights five points for action on mitigating the effects of climate change on public health for BIMSTEC states. Immediate measures range from setting aside differences, to addressing economic, political, and social concerns. Long-term solutions include knowledge-sharing, research and development, capacity building, and strengthening of frameworks. To engage in any of these activities, and indeed, tackle the threats posed by the challenges common to BIMSTEC nations, regional cooperation and diplomatic engagement are imperative. If harnessed fruitfully, the platform provided by the BIMSTEC can provide a range of innovative solutions for the challenges that lie ahead.
[1] BIMSTEC, established in 6 June 1997 through the Bangkok Declaration, is a regional organisation comprising of seven nations –Bangladesh, India, Myanmar, Sri Lanka, Thailand, Nepal and Bhutan –from South Asia and South East Asia.
[i] COAST Trust, Climate Change in the Bay of Bengal Region: Exploring Sectoral Cooperation for Sustainable Development, (Dhaka: Coastal Association for Social Transformation Trust, 2016).
[ii] Jacob Kumaresan, & Nalini Sathiakumar, “Climate change and its potential impact on health: a call for integrated action,” Bull World Health Organ 88 no.3, (March 2010): 163. doi: 10.2471/BLT.10.076034
[iii] Nicholas Watts et. al ,“Health and climate change: policy responses to protect public health,” The Lancet 386 no.10006 (7 November 2015): 1861-1914. doi:10.1016/s0140-6736(15)60854-6
[iv] “Summary” In Climate Change and Human Health: Risks and Responses, World Health Organization, 2003.
[v] Banalata Sen,,Meghnath Dhimal., Ashiath Thimna Latheef,, & Upasona Ghosh,“Climate change: health effects and response in South Asia.” BMJ, 359, (16 November 2017): j5117. doi: 10.1136/bmj.j5117
[vi] Manpreet Singh, Mala Rao & Colin D. Butler, “Climate change, health and future well-being in South Asia,” in Climate Change and Human Health Scenario in South and Southeast Asia ed. Rais Akhtar (Switzerland: SpringerCham, 2016) (pp. 11-27): doi: 10.1007/978-3-319-23684-1
[vii] Protecting Health From Climate Change, Department of Environment, 2008.
[viii] Daniel R. Taub, Brian Miller & Holly Allen, “Effects of elevated CO2 on the protein concentration of food crops: a meta‐analysis,” Global Change Biology, 14 no. 3, (27 November 2007) 565-575
[ix] Josef Schmidhuber, & Francesco N. Tubiello,“Global food security under climate change,” Proceedings of the National Academy of Sciences: 104 (50), (Dec 2007): 19703-19708; doi:10.1073/pnas.0701976104
[x] Arup Maharatna, "Food Scarcity and Migration: An Overview," Social Research: An International Quarterly 81, no. 2 (2014): 277-298. https://muse.jhu.edu/
[xi] Douglas K. Bardsley & Graeme J. Hugo “Migration and climate change: examining thresholds of change to guide effective adaptation decision-making,” Population and Environment, 32 no.2-3, (September 2010): 238-262. doi:10.1007/s11111-010-0126-9
[xii] Stellina Jolly & Nafees Ahmad, Climate Refugees in South Asia: Protection Under International Legal Standards and State Practices in South Asia (Singapore: Springer, 2018)
[xiii] Celia McMichael, John Barnett, & Anthony J. McMichael, “An ill wind? Climate change, migration, and health,” Environmental Health Perspectives 120 no. 5 (May 2012) 646-654 doi:10.1289/ehp.1104375
[xiv] Sayem Ahmed, Sylvia Szabo, & Kristine Nilsen “Catastrophic healthcare expenditure and impoverishment in tropical deltas: evidence from the Mekong Delta region.” International Journal for Equity in Health, 17:53 (April2018) doi: 10.1186/s12939-018-0757-5
[xv] World Development Indicators, World Bank, 2019.
[xvi] David Eckstein, Vera Künzel, & Laura Schäfer “Global climate risk index 2018.” (Bonn: Germanwatch e.V.,2017)
[xvii] Oomen C. Kurian, “Health policies of BIMSTEC states: The scope for cross-learning” ORF Issue Brief No. 211, November 2017, Observer Research Foundation.
[xviii] Fourth BIMSTEC Summit Declaration. BIMSTEC, 2018.
[xix] Status of the development of health national adaptation plan for climate change in South-East Asia, World Health Organization, 2017.
[xx] Ibid.
[xxi] Myanmar National Climate Change Policy, Strategy & Action Plan (NCCP and MCCSAP 2017-2030) Myanmar Climate Change Alliance, 2019.
[xxii] Myanmar Climate Change Strategy and Action Plan (MCCSAP) 2016–2030, MoNREC, 2017.
[xxiii] Climate and Health Country Profile – 2015 Sri Lanka, World Health Organization, 2016.
[xxiv] National Adaptation Plan for Climate Change Impacts in Sri Lanka 2016 to 2025, Climate Change Secretariat, 2015.
[xxv] Climate and Health Country Profile – 2015 Sri Lanka World Health Organization 2016.
[xxvi] Climate And Health Country Profile – 2015 Thailand World Health Organization, 2016.
[xxvii] Mohammad Masudur Rahman, & Chanwahn Kim, “Prospects for Economic Integration of BIMSTEC: Trade and Investment Scenario” International Journal of u-and e-Service, Science and Technology, Vol 9, no.4, (2016) 235-248.
[xxviii] Climate change and trade agreements: friends or foes?, Economist Intelligence Unit Report 2019.
[xxix] Gauri Noolkar-Oak, Geopolitics of Water Conflicts in the Teesta Basin, 2017.
[xxx] Fahida Khatun & Md Kamruzzaman,“Fiscal Implications of Rohingya Crisis for Bangladesh,” CPD Working Paper 120, October 2018, Centre for Policy Dialogue.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

MD Kamruzzaman is a Master in Public Policy Candidate and The Lee Foundation Scholar at the Lee Kuan Yew School of Public Policy National University ...
Read More +