
-
CENTRES
Progammes & Centres
Location
 PDF Download
PDF Download 
Shoba Suri, “Breakout Nation: The Nutrition Transformation of Bangladesh”, ORF Issue Brief No. 323, November 2019, Observer Research Foundation.
Introduction
Over the past few decades, South Asia has significantly improved its performance indicators in arresting undernutrition. Bangladesh, in particular, has made considerable progress in reducing undernutrition through scaling up nutrition-sensitive interventions like education and access to healthcare.[i] Bangladesh’s progress in this sector has set a positive trend for other nations in the region, especially India.
Since the early 1990s, Asia has been home to nearly three-fourths of the world’s poor. [ii] The consequences of poverty on children are well reflected in the high percentage of children who were stunted, wasting, and underweight in the region in 1990 (Table 1). One-third of children under the age of five in developing countries were underweight, in contrast to more than half in South Asia. The prevalence of underweight children widely varied within South Asia, with Bangladesh topping the list at 65.8 percent, followed by India (60.8). Wasting was prevalent in 17 percent of South Asian children, with disparities among Asian countries. Here again, three South Asian countries — India (18.9 percent), Bangladesh (15.5 percent) and Sri Lanka (12.9 percent) —contributed to the 56 percent of wasted children across Asia. Stunting prevalence was higher than underweight and wasting, with 41 percent in developing countries and a high 60 percent in South Asia. These numbers have improved over the years, but persistent problems indicate the need for deeper analysis of the nature of undernutrition in the region.
Table 1. Percentage of Wasted, Stunted and Underweight Children under five in 1990
| Region | Wasted | Stunted | Underweight |
| Developing Countries* | 9 | 41 | 34 |
| East & South East Asia | 5 | 33 | 24 |
| South Asia | 17 | 60 | 58 |
Source: Adapted from the FAO’s Sixth World Food Survey
The underlying factors[iii] for child undernutrition in Bangladesh include household food insecurity, poor healthcare services, and unhealthy household environments. Gender influences these underlying factors and affects both food security and caregiving. Water, sanitation, and health facilities influence the environment where children are exposed to infections and risk suffering undernutrition. Over the years, Bangladesh has made remarkable progress in its food availability and nutrition-sensitive interventions for access to clean drinking water and sanitation, infant and child mortality, immunisation coverage, and school enrollment. It needs to further mainstream the developments in the agriculture and health sectors for improved nutrition outcomes.[iv]
According to the Sustainable Development Goals Progress Report 2018,[v] Bangladesh has shown outstanding progress in the areas of poverty alleviation, ensuring food security, gender parity in primary and secondary level education, lowering infant and under-five mortality rate and maternal mortality ratio, improving immunisation coverage, and reducing the incidence of communicable diseases. Climate change poses a major threat to achieving the WHO’s global nutrition target 2025, with a direct link to stunting in children, caused by decrease in food availability and reduced resilience among the vulnerable population. According to the World Bank,[vi] climate change could accentuate poverty and inequality in South Asian countries. A study[vii] on the impact of climate-related shocks and stresses on nutrition and food security in Bangladesh conclude that flood events are associated with wasting and drought, with a rise in stunting.
The 2030 Sustainable Development Goals seek to end hunger and achieve food security and promote sustainable agriculture. This aims to reduce stunting among children and provide access to food through sustainable food systems. Bangladesh has been a frontrunner in achieving the Millennium Development Goals (MDGs) way ahead of 2015, and has strategies in place to achieve the SDGs. The progress is attributed to strong policies and programmes that promote access to universal education and quality maternal and child health services. However, challenges of high food insecurity, gender parity, and natural disasters need to be overcome to achieve the goals.
Poverty, Food Security, and Nutrition
A recent World Bank report[viii] shows sharp economic slowdown in South Asia due to a drop in domestic consumption. However, of all the countries in the region, Bangladesh (8 percent) and Nepal (7 percent) have shown upward growth projection as compared to India (6 percent), whose growth has dropped drastically. Table 2 summarises the GDP growth in South Asia along with projections for 2020-21.
Table 2. GDP growth in South Asia
| Country | 2018 | 2019 | 2020 | 2021 |
| Afghanistan | 1.8 | 2.5 | 3.0 | 3.5 |
| Bangladesh | 7.9 | 8.1 | 7.2 | 7.3 |
| Bhutan | 4.6 | 5.0 | 7.4 | 5.9 |
| India | 6.8 | 6.0 | 6.9 | 7.2 |
| Maldives | 6.7 | 5.2 | 5.5 | 5.6 |
| Nepal | 6.7 | 7.1 | 6.4 | 6.5 |
| Pakistan | 5.5 | 3.3 | 2.4 | 3.0 |
| Sri Lanka | 32 | 2.7 | 3.3 | 3.7 |
Source: Adapted from World Bank Report 2019, ‘Making Decentralization Work’
Bangladesh, with a population of approximately 163 million, is one of the world’s most densely populated countries. The country has made progress in reducing poverty from 34.8 percent in 2000 to 14.8 percent in 2016. It also has a developing market economy with a growth of 7.3 GDP, owing to garments exports and domestic agricultural sector.
Bangladesh ranks 88th out of 117 countries in the 2019 Global Hunger Index (GHI), and the share of its undernourished population is at 14.7 percent in 2016–2018.[ix] With a score of 25.8, the nation suffers from a serious level of hunger, even as numbers have improved over the decades. What is even more remarkable is the manner in which Bangladesh has pulled itself out of being a food-deficit country in the 1970s; today the country has food production at pace with its population growth.
The significant advancement in child nutrition in Bangladesh is attributed to its steady economic growth. The GHI indicates robust economic growth and attention to ‘nutrition-sensitive’ sectors such as education, sanitation, and health as being the key to Bangladesh’s success.[x] India, on the other hand, continues to grapple with a high rate of undernutrition.
The decline in stunting, for example, has been more significant in Bangladesh—from 58.5 percent in 1997 to 36 percent in 2014. In India, there has been a more marginal improvement over the same period, for both stunting (52 to 38.4 percent) and underweight (53.4 to 36 percent).[xi]
Bangladesh has also reduced stunting prevalence in the last three decades. However, there are still 5.5 million (36 percent) stunted children under the age of five (36 percent), and 14 percent children suffer from wasting. Evidence[xii] also suggests that over 70 percent of Bangladesh’s workforce was stunted in childhood, which has resulted in enormous economic costs to the nation. Undernutrition leads to long-term effects, including cognitive and growth deficits and a drop in immunity to infections. According to one study,[xiii] 80 percent of the world’s undernourished children are from only 20 countries, including Bangladesh.
To add to the burden of malnutrition in Bangladesh, 42 percent of women in the reproductive age are anaemic and 19 percent are underweight, which has lasting effects on future pregnancies, and is one of the leading causes for the high rate of low-birth weight babies.[xiv] The situation worsens when infants receive inadequate diets. According to the World Health Organization (WHO), an unbalanced diet and lack of food (other than mother’s milk), is directly linked to high rates of stunting, excessive weight, and death in children under five. Adolescent pregnancies and being underweight further increase both the risk of neonatal deaths and burden of low birth weight (23 percent). It is therefore important to break this intergenerational cycle of malnutrition. The first 1,000-day period from conception to two years of age provides a critical window of opportunity to prevent childhood stunting and obesity problems later in life. Exclusive breastfeeding, long considered the best form of nutrition for newborn babies, averages 42 percent globally whereas Bangladesh[xv] averages at 55 percent on exclusive breastfeeding and children who begin complementary feeding at 6 months is 65 percent. However, only 23 percent of children are fed minimum meal frequency and from 4+ food groups.
Progress to Date: Nutritional Outcomes
Figure 1: Malnutrition Trends (1997-2014)
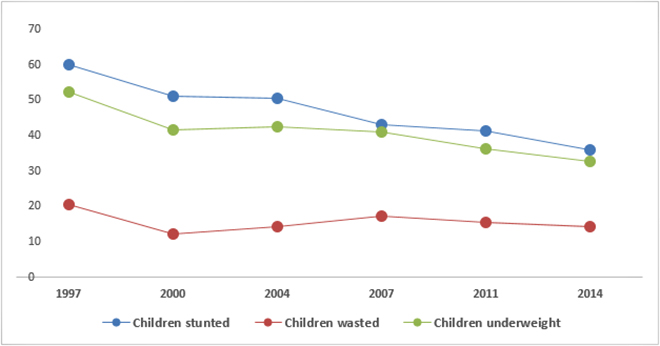
Figure 1 indicates the trends in the prevalence of malnutrition in Bangladesh over the years. The trends indicate massive decline over the two decades in children being stunted and underweight.
Stunting: There has been a steady decline in stunting among children in Bangladesh under five at the rate of 1.4 percentage per years; and yet, 36 percent of the nation’s children are stunted. The prevalence is high among children aged less than two years, indicating poor infant feeding and hygiene practices. There is a higher incidence of stunting in children in rural areas (38 percent) as compared to urban areas. The prevalence of stunting tends to increase more than twofold in parallel with maternal education. Stunting is at 47 percent for mothers with no formal education, and drops to a low of 18 percent with mothers who have received a secondary education. Stunting also shows a steady decline with increase in household income — with 19 percent in the highest quintile and a high of 49 percent in the lowest wealth quintile. There is regional/divisional disparity (Figure 2) in stunting rates ranging from high of 50 percent in Sylhet, much above the national average, to a low of 28 percent in Khulna.
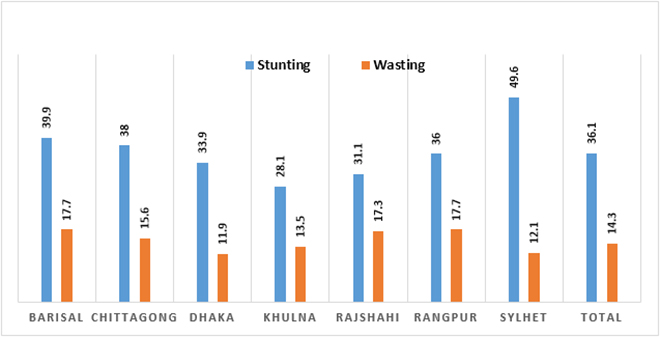
A recent study[xvi] on the prevalence of stunting across regional divisions of Bangladesh shows reduction in stunting across divisions — except Sylhet. The stunting has been on the higher side in Sylhet, 61 percent in 1996-97 to 49.6 percent in 2014, followed by 42 percent in Barisal and 41 percent in Chittagong. Dhaka was the only division with a 10 percent decline in stunting from 2011 to 2014, contributing to the overall reduction in stunting for Bangladesh. The regions/divisions of Bangladesh have distinct features — characterised by areas with frequent flooding, natural disasters, and hilly terrains — thus affecting the availability and accessibility of food. An earlier study[xvii] cites accumulation of wealth, improved parental education, and nutrition sensitive interventions of sanitation and health as important contributors in the reduction of malnutrition.
Wasting: According to WHO/UNICEF,[xviii] wasting is high at 14 percent in Bangladesh. The wasting prevalence has not shown much decline in the past two decades (Figure 1) — a slight improvement was observed in 2014. About 2.2 million children under five suffer from wasting and evidence[xix] suggests that a school feeding programme, along with school enrollment, can improve children’s diets. Unlike stunting, there is no difference in wasting rate across wealth quintile, ranging from 11-13. (Figure 2).
Figure 2: Stunting & Wasting across regions/divisions of Bangladesh
Underweight: The decline in rates of underweight children is similar to stunting, as is evident from Figure 1. According to a cross-country study,[xx] Bangladesh has had the fastest reductions in underweight and stunted children in the 1997-2007 period. However, with only 23 percent children aged between 6-23 months consuming a minimum acceptable diet, and a lack of availability of food — there is a risk of increasingly underweight children.
Anaemia: More than half of children under five (51 percent) are anaemic. A study[xxi] suggests that iron deficiency is a major cause of anaemia in children, followed by a deficiency of vitamin A (21 percent), zinc (45 percent), vitamin B12, and folate. Anaemia is high in children under the age of one (79 percent) and pregnant women. 42 percent of women in their reproductive age (15-49 years) are anaemic and this increases to 50 percent in pregnant women. Data indicates a deficiency of 22 percent (Vitamin B12) and 9 percent (folate) in non-pregnant/non-lactating women. Figure 3 highlights the prevalence in anaemia across age groups in children and women.
Figure 3: Presence of ‘Any Anaemia’ in 2014
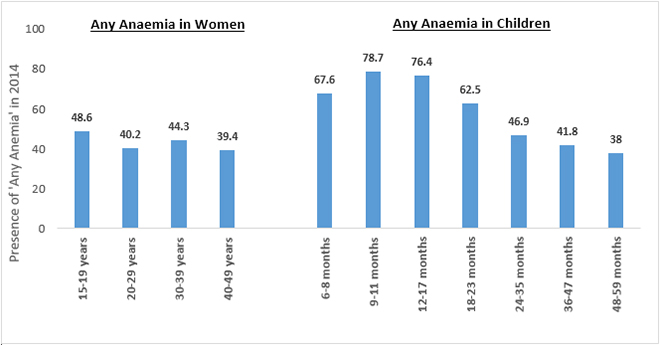
Maternal Malnutrition: Thirty-one percent of adolescent girls (15-19 years) and 19 percent of women (15-49 years) in Bangladesh are underweight, owing to poor maternal nutrition. This is contributing to an intergenerational cycle of malnutrition and poverty. Adolescent pregnancies are also associated with increased risk of stillbirths and neonatal deaths.[xxii] Maternal undernutrition and anaemia underlies the increased risk of low birth weight (23 percent) and subsequent stunting or wasting in children. On the other hand, obesity, or being overweight in 24 percent women of reproductive age (15-49 years), is a growing concern.
Maternity benefits are important for good health and nutrition for women after childbirth and also help establish exclusive breastfeeding. Bangladesh[xxiii] provides six months of paid maternity leave to women working in the public sector. While there is no provision for paternity leave or breastfeeding breaks, a breastfeeding room in the workplace is mandated. Unfortunately for the women in the private sector, in their case, this provision depends on the employer’s initiative. At present, there seems to be no provision for nearly 80 percent of women who work in the unorganized sector,[xxiv] primarily in garment factories.
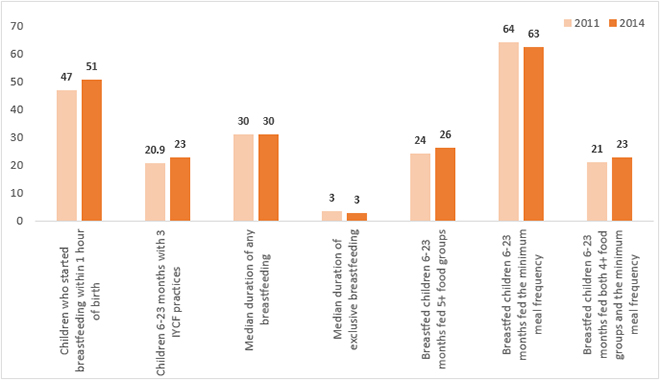
Infant and Young Child Feeding: Figure 4 indicates child nutrition practices. Exclusive breastfeeding at 0-5 months at 55 percent has dropped from 64 percent in 2011. Only half of all children in Bangladesh are exclusively breastfed and this contributes to the high rates of undernutrition. The early initiation of breastfeeding is at 51 percent with 27 percent receiving pre-lacteal feed. The prevalence is higher in rural areas (53 percent) than urban (47 percent) for early initiation and pre-lacteal feeding practice. The median duration of breastfeeding is estimated at 30 months. According to national data, the bottle-feeding rate of 14 percent is showing a decreasing trend over the years. Though 65 percent children between 6-23 months are introduced to complementary feeding, the minimum dietary diversity is only 23 percent. Only one-fourth of children receive a minimum acceptable diet with foods from 4+ food groups and frequency. The infant and young child feeding practices show variation in rural and urban communities. Sub-optimal feeding practices can increase risk of illness — leading to impaired growth and development. Studies[xxv] suggest lack of knowledge, time, and resources to the low rates of breastfeeding and complementary feeding, especially during floods. Improved education[xxvi] on complementary feeding along with behavioural change is necessary to improve feeding practices. It is also important to improve hygiene in calamity-prone areas to reduce morbidity related to poor feeding.
Figure 4: Status of Child Nutrition
Government Policies on Nutrition
Almost 25 million[xxxii] people go hungry every day in Bangladesh. The government is thus committed to improving maternal and child nutrition and has rolled out the National Plan of Action for Nutrition 2016-2025, coordinated by the National Nutrition Council. The plan is based on a multi-sectoral strategy involving health, education, agriculture, fisheries and livestock, environment, social protection, women empowerment, and disaster management to combat all forms of malnutrition. It aims to ensure universal access to nutrition services, and strengthened human resource capacity with focus on children, adolescent girls, pregnant women, and lactating mothers.
Over the past decade, the Government of Bangladesh has shown a strong commitment to reducing poverty, improving human development, and reforming its social protection system to address the high levels of malnutrition. The country has focused on nutrition-specific interventions that address the immediate causes of undernutrition. There have been various nutrition-specific policies implemented over the years since 1997. In 2011, the country adopted a multi-sector approach and integrated the nutrition services into the health sector through the Health, Population and Nutrition Sector Development Program to be implemented through the National Nutrition Service (NNS). The NNS coordinates across ministries including women and children, agriculture, disaster management to mainstream nutrition.
Efforts have also been made to develop social protection across the life cycle, with a greater focus on empowering women. The Government of Bangladesh is providing support for breastfeeding and complementary feeding, dietary diversification, food supplementation and fortification, and management of severe malnutrition at the community level. The government of Bangladesh programme on the ‘National Strategy for Anemia Prevention and Control’ further aims to improve maternal and child nutrition for anaemia reduction by dietary improvement and fortification.
Strategies to improve Food Security
Bangladesh has worked on an innovative approach to impact food and nutrition security. The nutrition garden strategies have shown considerable impact in improving food production, consumption, and nutrition. An intervention[xxxiii] from Bangladesh found a three- to four-fold increase in variety and quantity of fruits and vegetables among households practicing kitchen gardens. A home garden model[xxxiv] tested in rural households in Bangladesh has found a reduced expense on vegetables, improved intake of fresh fruits and vegetables, and increased income generation by sale of the produce. Aquaculture and fish consumption,[xxxv] being common in Bangladesh, provide for the micronutrients and protein needs of children and women. Child mortality has been found to be lower in Bangladesh during fishing seasons in mothers who consume fish. According to a study,[xxxvi] 25 percent of the recommended nutrient intake is fulfilled for infants, pregnant and lactating women with consumption of fish in Bangladesh. Micronutrients and Omega 3 fatty acids help reduce malnutrition and burden of non-communicable diseases. Research[xxxvii] findings on leveraging agriculture for nutrition in South Asia suggest pathways linking nutrition and agriculture and highlight its role in achieving the SDG on No Poverty.
Conclusion
Stunting remains a considerable challenge in Bangladesh. There is a need for improving the coverage of the first 1,000 days for pregnant women and adolescent girls to break the intergenerational cycle of malnutrition. Bangladesh faces the challenge of food insecurity, access to affordable quality of nutritious food, and dietary diversity especially in rural areas. Infant and young child feeding practices are presently inadequate, but are critical for tackling malnutrition. However, the improvements in access to safe water and sanitation have reduced open-defecation, leading to a reduction in stunting. Bangladesh is tackling malnutrition by addressing both direct and underlying causes that affect nutrition.
The Government of Bangladesh, through its multi-sectoral approach and coordinated action with other stakeholders, is committed to achieve the SDG targets by 2030. The country is setting an example in tackling undernutrition for others with similar demographics and nutritional status. What is needed is effective and sustained implementation and scaling up of both nutrition-specific and nutrition-sensitive interventions to tackle hunger and malnutrition. A potential programme should have robust monitoring and evaluation systems to show the impact on nutrition. The integration of women, behaviour change communication strategies, and income-generating activities can encourage sustainable outcomes for nutrition in Bangladesh.
Endnotes
[i] Nisbett, Nicholas, Peter Davis, Sivan Yosef, and Nazneen Akhtar. “Bangladesh’s story of change in nutrition: Strong improvements in basic and underlying determinants with an unfinished agenda for direct community level support.” Global food security 13 (2017): 21-29.
[ii] Food and Agriculture Organization of the United Nations (FAO) Rome 1996. The Sixth World Food Survey.
[iii] Longhurst, Richard, Inka Barnett, and Nabeela Ahmed. Determinants of Child Undernutrition in Bangladesh: Literature Review. No. id: 7910. 2015.
[iv] Naher, Firdousi, Barkat-e-Khuda, Shaikh Shamsuddin Ahmed, and Mahabub Hossain. “How nutrition-friendly are agriculture and health policies in Bangladesh?.” Food and nutrition bulletin 35, no. 1 (2014): 133-146.
[v] Bangladesh Planning Commission. Sustainable Development Goals. Bangladesh First Progress Report 2018.
[vi] Mani, Muthukumara, Sushenjit Bandyopadhyay, Shun Chonabayashi, Anil Markandya, and Thomas Mosier. South Asia’s Hotspots: The Impact of Temperature and Precipitation Changes on Living Standards. The World Bank, 2018.
[vii] Béné, C., J. Waid, M. Jackson-deGraffenried, A. Begum, M. Chowdhury, V. Skarin, A. Rahman et al. “Impact of climate-related shocks and stresses on nutrition and food security in selected areas of rural Bangladesh.” Dhaka, the World Food Programme (2015): 3.
[viii] World Bank. 2019. “Rethinking Decentralization” South Asia Economic Focus (October), World Bank, Washington, DC.
[ix] Global Hunger Index 2019.
[x] Ibid
[xi] National Family Health Survey 4 2015-16.
[xii] Galasso, Emanuela, and Adam Wagstaff. “The aggregate income losses from childhood stunting and the returns to a nutrition Intervention aimed at reducing stunting.” Economics & Human Biology (2019).
[xiii] Bryce, Jennifer, Denise Coitinho, Ian Darnton-Hill, David Pelletier, Per Pinstrup-Andersen, and Maternal and Child Undernutrition Study Group. “Maternal and child undernutrition: effective action at national level.” The Lancet 371, no. 9611 (2008): 510-526.
[xiv] Figueiredo, Ana CMG, Isaac S. Gomes-Filho, Roberta B. Silva, Priscilla PS Pereira, Fabiana AF Da Mata, Amanda O. Lyrio, Elivan S. Souza, Simone S. Cruz, and Mauricio G. Pereira. “Maternal anemia and low birth weight: a systematic review and meta-analysis.” Nutrients 10, no. 5 (2018): 601.
[xv] UNICEF 2019. State of World Children. Children, food and nutrition.
[xvi] Saha, Unnati Rani, Aparajita Chattapadhayay, and Jan Hendrik Richardus. “Trends, prevalence and determinants of childhood chronic undernutrition in regional divisions of Bangladesh: Evidence from demographic health surveys, 2011 and 2014.” PloS one 14, no. 8 (2019): e0220062.
[xvii] Headey, Derek, John Hoddinott, Disha Ali, Roman Tesfaye, and Mekdim Dereje. “The other Asian enigma: explaining the rapid reduction of undernutrition in Bangladesh.” World Development 66 (2015): 749-761.
[xviii] WHO & UNICEF 2017. REPORT of The Fourth Meeting of the WHO-UNICEF Technical Expert Advisory group on nutrition Monitoring (TEAM).
[xix] Ahmed, Akhter U. “Impact of feeding children in school: Evidence from Bangladesh.” Washington, DC: International Food Policy Research Institute (2004).
[xx] Headey, Derek D. “Developmental drivers of nutritional change: a cross-country analysis.” World Development 42 (2013): 76-88.
[xxi] ICDDR B, UNICEF (Bangladesh), GAIN, Institute of Public Health and Nutrition. “National micronutrients status survey 2011–12.” (2013).
[xxii] National Nutrition Services (NNS) and Institute of Public Health Nutrition (IPHN). Directorate General of Health Services Ministry of Health & Family Welfare, Government of Bangladesh. National Low Birth Weight Survey 2015.
[xxiii] World Breastfeeding Trends Initiative. Bangladesh Assessment Report 2015 of Infant and Young Child Feeding Policies and Programmes.
[xxiv] Fatema-tuj-zuhra. Significance of Maternity benefits: Bangladesh perspectives. IOSR Journal Of Humanities And Social Science (IOSR-JHSS) Volume 21, Issue 5, Ver. 1 (May. 2016) PP 01-07.
[xxv] Goudet, Sophie M., Paula L. Griffiths, Barry A. Bogin, and Nasima Selim. “Impact of flooding on feeding practices of infants and young children in Dhaka, Bangladesh Slums: what are the coping strategies?.” Maternal & child nutrition 7, no. 2 (2011): 198-214.
[xxvi] Manikam, Logan, Alexandra Robinson, Jia Ying Kuah, Hrisheekesh J. Vaidya, Emma C. Alexander, George W. Miller, Kunjshri K. Singh et al. “A systematic review of complementary feeding practices in South Asian infants and young children: the Bangladesh perspective.” BMC Nutrition 3, no. 1 (2017): 56.
[xxvii] Rajia, Sultana, Md Sabiruzzaman, Md Kamrul Islam, Md Golam Hossain, and Pete E. Lestrel. “Trends and future of maternal and child health in Bangladesh.” PloS one 14, no. 3 (2019): e0211875.
[xxviii] World Bank. “Promising Progress: A Diagnostic of Water Supply, Sanitation, Hygiene, and Poverty in Bangladesh.” (2018).
[xxx] ibid
[xxxi] General Economics Division Planning Commission Government of the People’s Republic of Bangladesh. Development Planning in Bangladesh: 7th Five Year Plan and SDG Implementation 2016.
[xxxii] FAO, IFAD, UNICEF, WFP and WHO. 2018. The State of Food Security and Nutrition in the World 2018. Building climate resilience for food security and nutrition. Rome, FAO.
[xxxiii] Talukder, A., N. J. Haselow, A. K. Osei, E. Villate, D. Reario, H. Kroeun, L. SokHoing, A. Uddin, S. Dhunge, and V. Quinn. “Homestead food production model contributes to improved household food security and nutrition status of young children and women in poor populations. Lessons learned from scaling-up programs in Asia (Bangladesh, Cambodia, Nepal and Philippines).” Field Actions Science Reports. The Journal of Field Actions Special Issue 1 (2010).
[xxxiv] Ferdous, Zannatul, Avishek Datta, Anil Kumar Anal, Mazharul Anwar, and ASM Mahbubur Rahman Khan. “Development of home garden model for year round production and consumption for improving resource-poor household food security in Bangladesh.” NJAS-Wageningen Journal of Life Sciences 78 (2016): 103-110.
[xxxv] Bennett, Abigail, Pawan Patil, Kristin Kleisner, Doug Rader, John Virdin, and Xavier Basurto. Contribution of Fisheries to Food and Nutrition Security: Current Knowledge, Policy, and Research. Duke University, Nicholas Institute for Environmental Policy Solutions, 2018.
[xxxvi] Bogard, Jessica R., Shakuntala H. Thilsted, Geoffrey C. Marks, Md Abdul Wahab, Mostafa AR Hossain, Jette Jakobsen, and James Stangoulis. “Nutrient composition of important fish species in Bangladesh and potential contribution to recommended nutrient intakes.” Journal of Food Composition and Analysis 42 (2015): 120-133.
[xxxvii] Gillespie, Stuart, Nigel Poole, Mara van den Bold, R. V. Bhavani, Alan D. Dangour, and Prakash Shetty. “Leveraging agriculture for nutrition in South Asia: What do we know, and what have we learned?” Food Policy 82 (2019): 3-12.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Dr. Shoba Suri is a Senior Fellow with ORFs Health Initiative. Shoba is a nutritionist with experience in community and clinical research. She has worked on nutrition, ...
Read More +



