Shoba Suri and Laetitia Warjri, “A Primer on Serology (Antibody) Testing,” ORF Special Report No. 114, July 2020, Observer Research Foundation.
GLOSSARY
1. Assay
The measurement of the presence of a chemicaland its amount.
2. Certification for In-Vitro Diagnostic devices (CE-IVD)
‘CE marking’ indicates that an IVD device complies with the European In-Vitro Diagnostic Devices Directive (98/79/EC), issued by the European Parliament, certifying that the device may be legally commercialised in the EU. Such marking is required for all in vitro diagnostic (IVD) devices sold in Europe[1].
3. Coronavirus (CoV)
A group of viruses that cause diseases in humans[2]and animals. They have been named thus as when viewed under a microscope, they resemble a corona[3]—the bright crown-like ring of gases surrounding the sun that is visible during a solar eclipse.
4. Emergency Use Authorisation (EUA)
A provision[4]that enables the drug regulator to allow unapproved medical products or unapproved uses of approved medical products in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions caused by CBRN (Chemical, biological, radiological and nuclear) threat agents when there are no adequate, approved, and available alternatives.
5. Immunoglobulin G (IgG)
Immunoglobulin G[5]is the “workhorse” of systemic humoral immunity, since it is the isotype most commonly found in the blood and tissues.
6. Immunoglobulin M (IgM)
Immunoglobulin M[6]is the first immunoglobulin synthesised by neonates. Its molecules are the preponderant class of immunoglobulin molecules appearing during early phases of immune responses.
7. Infection Fatality Rate (IFR)
The infection fatality rate[7]indicates the proportion of deaths among those found to have an infectious disease.
8. Polymerase Chain Reaction (PCR)
Polymerase Chain Reaction is a technique to make copies[8]of a specific DNA region in vitro in a lab setting (in a test tube rather than in an organism).
9. Polymerase Chain Reaction with Reverse Transcription (RT-PCR)
Reverse transcription polymerase chain reaction[9]is a technique to detect or quantify RNA. It uses a reverse transcriptase enzyme to convert RNA to DNA, followed by PCR to amplify the DNA.
10. Real Time Quantitative Reverse Transcription PCR (RT-qPCR)
Real-Time Quantitative Reverse Transcription PCR[10]is a major development of PCR technology that enables reliable detection and measurement of products generated during each cycle of the PCR process.
11. Sensitivity
“Analytical sensitivity”[11]represents the smallest amount of a substance in a sample that can accurately be measured by an assay. A 100 percent sensitive test would mean there are no false negatives.
12. Seroprevalence
The overall occurrence of a disease or condition within a defined population at one time, as measured by blood tests (serologic tests).
13. Severe Acute Respiratory Syndrome Corona Virus 2 (SARS-CoV-2)
The name of the virus responsible for the development of COVID-19, or Corona Virus Disease 2019.
14. Specificity
“Analytical specificity”[12]refers to the ability of an assay to measure one particular organism or substance, rather than others, in a sample. A 100 percent specific test would mean there are no false positives.
SEROLOGY (ANTIBODY) TESTING FOR COVID-19
WHAT IS SEROLOGY (ANTIBODY) TESTING?
According to the Johns Hopkins Centre for Health Security,[13]“Serology tests are blood-based tests that can be used to identify whether people have been exposed to a particular pathogen by looking at their immune response.” Serology tests, also known as antibody tests, reveal in detail the prevalence of a particular disease in the population.
TYPES OF SEROLOGY (ANTIBODY) TESTING
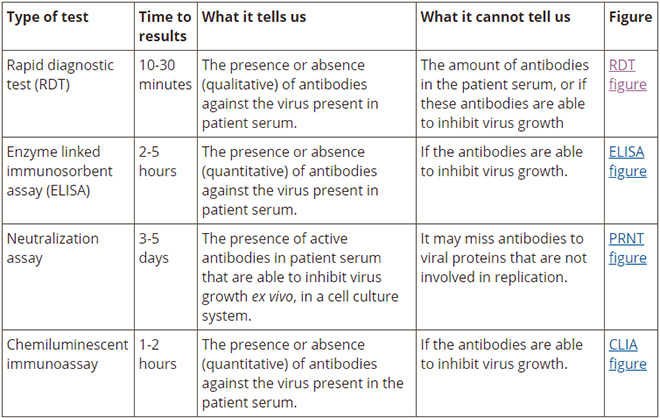
There are four kinds of antibody tests that are most commonly used: Rapid diagnostic test (RDT), Enzyme-linked immunosorbent assay (ELISA), Neutralisation assay, and Chemiluminescent immunoassay (CLIA).
Source:Johns Hopkins Centre for Health Security[14]
UNDERSTANDING ANTIBODY TESTING
A study by the U.S. Food and Drug Administration (FDA) on the first batch of COVID-19 antibody diagnostics shows[15]the serology test’s approximate ability to avoid false-positive and false-negative results (specificity and sensitivity, respectively), and their overall predictive value. In May, the Indian Council of Medical Research[16](ICMR) also approved two COVID-19 antibody test kits—for detecting IgG and IgM antibodies—and stated that these tests were a valuable resource in community screening and surveillance.
According to the US FDA,[17]“The performance of antibody tests is measured by their “sensitivity”, or their ability to identify those with antibodies to SARS-CoV-2 (true positive rate); and their “specificity”, or their ability to identify those without antibodies to SARS-CoV-2 (true negative rate)”. A calculator[18]developed by the FDA, shows predictive values based on different levels of prevalence, which can change with time or location.
Anotherstudy[19]on antibody responses in patients with COVID-19 has found that serological testing helps in diagnosing suspected cases with negative RT–PCR and identifying asymptomatic infections. Yet another study[20]on SARS-CoV-2 IgG antibody responses in New York City showed a positivity rate of 44 percent among 28,523 cases. This revealed the extensive prevalence of the pandemic in the city. The highest rate of prior infection was seen in the age group of 11-20 years. This could probably be because of a strong immune response in younger age groups.
Another non peer-reviewed study[21]to test if the seroprevalence estimates were biased, has suggested that assays with imperfect sensitivity undermine the extent of true seroprevalence, as antibody levels peak a few weeks after infection, and reduce gradually. Optimisation and validation of serological assays should involve samples from across the spectrum of severity, as well as time since the infection.
The following variables need to be taken into account while developing antibody tests:
1. Test the Tests: It is important to check the accuracy of the tests in distinguishing between people who have had the disease and those who have not. A test with more than 99-percent sensitivity and specificity, with only one false positive or negative can be said to be of good quality. An analysis[22]has shown that specificity of some COVID-19 tests can be as low as 40 percent, with sensitivity ranging from 67 to 93 percent. More accurate tests have been developed since.
2.Timing Is Critical: The link between the timing of a test and its accuracy is crucial. The antibodies need time to develop and will not be detected if the test is conducted too soon after the onset of infection. There is a possibility of false positives too if the test uses antigens that not only identify SARS-CoV-2 but other strains of virus as well. This has been demonstrated in an analysis[23] to validate serologic assays useful for patient contact tracing, serosurveillance and vaccine evaluation studies.
3. Infection versus Immunity:A non-peer-reviewedstudy on 175 people from China showed mild symptoms, and varied levels of antibodies being produced in their bodies following a COVID-19 infection. It was not clear whether they had the immunity to protect them from the next bout of attack of the virus. However, in another recent study[24]on COVID-19 recovered patients, cellular and humoral immunity and high levels of IgG antibodies were detected.
APPROVED ANTIBODY TESTS, COUNTRY-WISE
The following are some of the tests that have been approved for diagnostic use and research, and for surveillance purposes, in different countries:
Country
Type of test
Sensitivity
Specificity
Phase of development
US/China
RDT
93.8
95.6
Approved by FDA for Emergency Use Authorisation (EUA) on diagnostics
US
RDT
95.7% (IgM) and 99% (IgG)
99% (Both)
Approved by FDA for EUA
US
ELISA
90-97%
98%
Approved by FDA for EUA
US
Modified ELISA
98%
99%
Received EUA
US/Switzerland
ECLIA
(Electrochemiuminescence Immunoassay Analyzer)
From 0-6 days, 65.5%; from 7-13 days, 88.1%; from 14 days onward, 100%
99.81%
Received EUA
Germany
ELISA
From 0-10 days, 13.9%; from 11-20 days, 61.1%; from 21 days onward, 100%. 90% by the National Cancer Institute (NCI) validation
60.7% (0-6 days post PCR positive), 97.5% (7-13 days post PCR positive), 100% (14+ days post PCR positive).
99.82%
Received EUA
US
CLIA
65.1% (0-6 days post PCR positive),97.5% (7-13 days post PCR positive), 100% (14+ days post PCR positive).
99.81%
Received EUA
US
CLIA
98.1%
98.6%
Received EUA
US
ECLIA
84%
63%
Received EUA and CE/IVD
China
RDT
92.5% (IgM), 91.56% (IgG)
98.1% (IgM), 99.52% (IgG)
Received EUA
Singapore
Neutralisation assay
90%
Deployed in Singapore
Switzerland
Multiplexed Immuno-Refractive Assay (MIRA)
100%
99.8%
CE/IVD
UK
RDT
100%
98.7%
Received CE/IVD
Mexico
RDT
99.9% (IgG) 85% (IgM)
98% (IgG) 96% (IgM)
Received CE/IVD, emergency use in Mexico, Brazil,etc.
Source: Johns Hopkins Centre for Health Security[25]
CLINICAL STUDIES TO EVALUATE ANTIBODY TESTING KITS
The US’ National Covid Testing Scientific Advisory Panel conducted a study[26]called “Evaluation of antibody testing for SARS-CoV-2 using ELISA and lateral flow immunoassays”. The authors developed an ELISA test in-house, which used the recombinant SARS-CoV-2 trimeric spike protein. It tested for IgM and IgG antibodies against RT-qPCR. The results showed 100 percent sensitivity for IgG ten days after the onset of symptoms in 31 samples.
Another study,[27]conducted in Japan, on IgM and IgG antibodies in COVID-19 patients, found IgM in 95.8 percent of positive cases, while IgG was detected in 62.5 percent of cases after two weeks.
This study[28]attempted to improve upon ELISA-based testing methods. The scientists used a protein microarray[2]that allowed for pooling (or multiplexing) of samples. In this case, dried blood spots were used. In a total of 1,576 cases, the authors found 158 positive and 1,418 negative samples. The overall sensitivity varied. In this study, the sensitivity/specificity was reported with all antigens and antibodies combined (versus isolating certain antigens and protein spikes). No cross-reactivity to antibodies formed in response to other corona viruses was found.
The study[29]measured the total antibodies to SARS-CoV-2 based on a Single Molecule Array (Simoa) assay. In other cases, the Simoa Protocol has shown a 1,000-fold improvement in sensitivity over a standard ELISA test. It also allows for the analysis of multiple types of antigens and antibodies at the same time (and not in isolation).
This group[30]tested for IgM and IgG antibodies to the SARS-CoV Rp3 nucleocapside (N) protein in 16 Covid-19 patients, developing an in-house ELISA test to do so. On day five, it was found that 81 percent of patients were positive for IgM antibodies and 100 percent for IgG antibodies.
This study[31]found that, for large-scale sero-epidemiology studies, using IgG based ELISA testing on the receptor binding domain (RBD) of the spike protein to screen sera for SARS-CoV-2 antibodies, followed by confirmation using plaque reduction neutralisation tests (PRNT90), is a valid approach.
ANTIBODY TESTING ACROSS COUNTRIES
According to the UK’s Public Health Corona Virus Disease Weekly Surveillance Report of Week 21[32](May 18 to May 24), about five percent of people across England and 17 percent in London tested positive for antibodies, as per antibody surveillance. The UK plans[33]to roll out millions of coronavirus antibody tests approved by Public Health England, as announced on May 22 by the its Health Secretary Matt Hancock. The pharmaceutical giant Roche[34]has stated that its test has specificity greater than 99.8 percent and sensitivity of 100 percent 14 days after a person has tested positive for COVID-19 through a polymerase chain reaction (PCR) swab test, which detects whether someone has the virus or not.
The US FDA has authorised emergency use for the sale of antibody tests (as mentioned in Table 1). A clinical study[35]found the tests, conducted two weeks after the symptoms arose, had more than 99.6 percent specificity and 100 percent sensitivity.
Germany has already rolled out antibody tests across the country and is conducting studies to determine how much of its population has been infected by COVID-19. One of its studies[36]found 14 percent of the population had previously been infected and had immunity.
Australia has reportedly spent almost $19 million buying one million antibody tests, which, however, were found inaccurate with high rates of false positives as per the Australian National University. The kits were procured from pharmaceutical companies[37]and laboratories across China, South Korea and the US.
China’s testing in Wuhan[38]to determine seroprevalence was carried out on about 17,000 people, including healthcare workers, factory workers and community residents. The seroprevalence was 3.2-3.8 percent, and decreased in other cities away from the epicentre. A multi-cohort[39]study on the seroprevalence of SARS-CoV-2 in Hong Kong and Hubei provinces found four percent had COVID-19 antibodies. The low seroprevalence shows the lack of herd immunity, making Hong Kong and Hubei vulnerable to a recurrence of SARS-CoV-2.
Canada[40]plans to collect and test at least one million blood samples over the next two years to track the virus in the general population and other at-risk groups, such as the elderly and healthcare workers.
Gibraltar,[41]with a population of 33,700, will be the first country to carry out COVID-19 antibody tests on its entire population.
The Japan Sumo Association has planned[42]antibody testing on all its 1,000 members, including wrestlers and referees. The results are yet to be declared.
WHAT SEROSURVEYS FROM DIFFERENT COUNTRIES REVEAL
From March to May this year, multiple serosurveys were carried out in different countries and regions. The results of some of the major ones are provided below.
COVID-19 seroprevalence of antibodies in Santa Clara County in the US[43]was 2.49 to 4.16 percent by early April. This indicates a manifold increase (50 to 85 times) compared to confirmed cases.
Approximately 4.1 percent of the US’ Los Angeles County’s[44]adult population had antibodies to the virus. In absolute terms, approximately 221,000 to 442,000 adults in the county have had COVID-19. These estimates are much higher (28 to 55 times) than the confirmed cases (7,994), as of early April.
A state survey found that about 21 percent of people in New York City[45]had coronavirus antibodies, while about 17 percent on Long Island did. Westchester and Rockland counties had 12 percent, while in the rest of New York State, less than four percent had antibodies.
Miami-Dade researchers[46]partnering with Florida Power & Light, called on people to volunteer for testing at their drive-through testing locations. About six percent[47] of the 1,400 tested showed presence of antibodies. The survey matched the national trend of African-Americans being disproportionately more impacted[48]by the novel coronavirus than other ethnicities.
The municipality of Gangelt[49]in Germany, near the Netherlands border, was hit hard by COVID-19 after a carnival celebration in February. Antibody tests showed 14 percent of the population have developed antibodies.
In Helsinki, Finland, the number of coronavirus infections is believed to be much more than the laboratory infections identified. Coronavirus antibodies[50]were detected in 0.7 to 3.4 percent of samples during a three-week study of a small (147) sample size. (It takes about two weeks for antibodies to form so that variation can be seen).
Randomised COVID-19 serology surveys[51]from Scotland,[52]Denmark and Finland show seroprevalence of 1.2, 1.8, and 3.4 percent, respectively. However, the Infection Fatality Rate (IFR) in Denmark is estimated at only 0.21 percent, and is seven times lower for Finland and Scotland – which leads to questions about the quality of these countries’ data, their death records, whether their survey resolution was insufficient or they conducted surveys too early. The survey suggests some conditions to correctly determine IFR from serology tests. For instance, the serology test has to coincide either with the peak of death incidence or should have been taken after that, as the time lag for seroprevalence—15.4 days—is comparable to the time lag for death to occur. Also, serology testing should be statistically designed so as to be representative of the population.
Of the 40,000 tested in Russia in May 2020,[53]14 percent had antibodies. One out of seven healthy Russians may be infected with SARS-CoV-2. The tests have 95 percent sensitivity and 98 percent specificity for an antibody that develops up to four weeks after people first came in contact with the virus.
Spain[54]has been one of the worst hit in terms of deaths and devastation. Only five percent of the 70,000 people tested in Spain showed presence of antibodies as of mid-May. This puts the majority of the population at risk, as lifting of restrictions can lead to a rise in cases. The study was carried out by the Carlos III Institute for Health and Spain’s National Statistics Institute on 36,000 randomly selected households. Only about 10-14 percent of the population in and around Madrid[55]was found to have antibodies. Only seven percent of Barcelona’s[56] population showed the presence of antibodies. The numbers became smaller outside of these two major cities. Herd immunity seems far off for the Spanish population.
In India,[57]an unpublished serosurvey showed that 15-30 percent of the population within containment zones and hotspots have developed antibodies. The report revealed that the infection rate was higher in cities such as Mumbai, Pune, Delhi, Ahmedabad and Indore. The samples were collected from 10 hotspot cities and 60 districts, which together account for 70 percent of India’s cases. ELISA-based antibody testing kits[58]developed in India by the National Institute of Virology were used for the antibody survey.
LIMITATIONS TO SEROLOGY (ANTIBODY) TESTING
There are limitations to serology (antibody) testing which could have serious implications while understanding the results. Some of these limitations have been highlighted by the American Medical Association:[59]
False positive results: There are challenges in understanding positive results when the prevalence of the disease in a population at a given time is low. There could be increased chances of false positive results even when tests with high sensitivity and specificity are used.
Cross-reactivity: This is a possibility, where the test detects not only antibodies to the novel coronavirus (COVID-19), but also other strains that cause the common flu. Such tests wrongly add to the number of positive cases.
Immunity status: There is no evidence of immunity to COVID-19 after having the infection. As this is a novel strain of virus, not much is known and little data is available to understand the immunity status of the COVID-19 strain.
STRATEGIES and GUIDELINES
Guidelines[60]for the validation and batch testing of COVID-19 diagnostic kits have been developed by India’s ICMR. They maintain that the test can be carried out on blood/serum/plasma samples, and shows positive results for several weeks after infection. However, a negative test does not rule out COVID-19 infection.
ICMR has also developed a strategy for COVID-19 testing in India[61]. The strategy includes testing of all symptomatic influenza-like illness (ILI) among returnees and migrants within seven days of the illness. All symptomatic health and frontline workers involved in containment and mitigation of COVID-19 will be tested.
Anational strategy[62]has been developed by Johns Hopkins Centre for Health Security for serology/antibody testing in the US. Serology tests for the SARS-CoV-2 virus can be helpful in making informed public health decisions during the pandemic. It is possible that not all who get infected by SARS-CoV-2 are tested before the virus is cleared from their bodies and they can also be asymptomatic. Thus, it is important to know the seroprevalence in a population and the extent of antibody testing needed to reach reliable conclusions. There also needs to be a check on the accuracy, validity and comparability of the available tests.
Endnotes
[1]A microsphere immunoassay is a test used for the detection of serum antibodies to avian influenza virus.
[2]A microarray is a laboratory tool used to detect the expression of thousands of genes at the same time.
[11]Saah, Alfred J., and Donald R. Hoover. ““Sensitivity” and “specificity” reconsidered: the meaning of these terms in analytical and diagnostic settings.” (1997): 91-94.
[19]Long, Quan-Xin, Bai-Zhong Liu, Hai-Jun Deng, Gui-Cheng Wu, Kun Deng, Yao-Kai Chen, Pu Liao et al. “Antibody responses to SARS-CoV-2 in patients with COVID-19.” Nature medicine (2020): 1-4.
[20]Reifer, Josh, Nosson Hayum, Benzion Heszkel, Ikey Klagsbald, and Vincent A. Streva. “SARS-CoV-2 IgG Antibody Responses in New York City.” medRxiv (2020).
[22]Lassaunière, Ria, Anders Frische, Zitta B. Harboe, Alex CY Nielsen, Anders Fomsgaard, Karen A. Krogfelt, and Charlotte S. Jørgensen. “Evaluation of nine commercial SARS-CoV-2 immunoassays.” Medrxiv (2020).
[23]Okba, Nisreen MA, Marcel A. Müller, Wentao Li, Chunyan Wang, Corine H. GeurtsvanKessel, Victor M. Corman, Mart M. Lamers et al. “Severe acute respiratory syndrome coronavirus 2-specific antibody responses in coronavirus disease 2019 patients.” Emerging infectious diseases 26, no. 7 (2020).
[24]Ni, Ling, Fang Ye, Meng-Li Cheng, Yu Feng, Yong-Qiang Deng, Hui Zhao, Peng Wei et al. “Detection of SARS-CoV-2-specific humoral and cellular immunity in COVID-19 convalescent individuals.” Immunity (2020).
[26]Adams, Emily R., Rekha Anand, Monique I. Andersson, Kathryn Auckland, J. Kenneth Baillie, Eleanor Barnes, John Bell et al. “Evaluation of antibody testing for SARS-Cov-2 using ELISA and lateral flow immunoassays.” (2020).
[27]Imai, Kazuo, Sakiko Tabata, Mayu Ikeda, Sakiko Noguchi, Yutaro Kitagawa, Masaru Matuoka, Kazuyasu Miyoshi et al. “Clinical evaluation of an immunochromatographic IgM/IgG antibody assay and chest computed tomography for the diagnosis of COVID-19.” Journal of Clinical Virology (2020): 104393.
[28]Krishnamurthy, Hari K., et al. “Antibody Profiling and Prevalence in the US population during the SARS-CoV2 Pandemic.” medRxiv (2020).
[29]Norman, Maia, et al. “Ultra-Sensitive High-Resolution Profiling of Anti-SARS-CoV-2 Antibodies for Detecting Early Seroconversion in COVID-19 Patients.” medRxiv (2020).
[30]Zhang, Wei, et al. “Molecular and serological investigation of 2019-nCoV infected patients: implication of multiple shedding routes.” Emerging microbes & infections 9.1 (2020): 386-389.
[31]Perera, Ranawaka APM, et al. “Serological assays for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), March 2020.” Eurosurveillance 25.16 (2020): 2000421.
[38]Xu, Xin, Jian Sun, Sheng Nie, Huiyuan Li, Yaozhong Kong, Min Liang, Jinlin Hou et al. “Seroprevalence of immunoglobulin M and G antibodies against SARS-CoV-2 in China.” Nature Medicine (2020): 1-3.
[39]To, Kelvin Kai-Wang, Vincent Chi-Chung Cheng, Jian-Piao Cai, Kwok-Hung Chan, Lin-Lei Chen, Lok-Hin Wong, Charlotte Yee-Ki Choi et al. “Seroprevalence of SARS-CoV-2 in Hong Kong and in residents evacuated from Hubei province, China: a multicohort study.” The Lancet Microbe (2020).
[40]Canada’s first antibody test marks step forward in COVID-19 response
[43]Bendavid, Eran, Bianca Mulaney, Neeraj Sood, Soleil Shah, Emilia Ling, Rebecca Bromley-Dulfano, Cara Lai et al. “COVID-19 Antibody Seroprevalence in Santa Clara County, California.” MedRxiv (2020).
[51]Hegarty, Ronan. “Evidence summary: What seroprevalence studies have been completed in other countries-general population studies and also studies on specific population sub-groups such as health workers, hospitalized patients, blood donors and children?[v1. 0].”
[58]Press Release. Indian Council of Medical Research & National Institute of Virology ‘“COVID KAVACH ELISA” for antibody detection for COVID-19’. May 14 2020.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Dr. Shoba Suri is a Senior Fellow with ORFs Health Initiative.
Shoba is a nutritionist with experience in community and clinical research. She has worked on nutrition, ...
Laetitia Bruce Warjri is a Head of Communications and Outreach at ORF.
Before joining ORF, Laetitia worked as a journalist with the India Today Group and ...

 PDF Download
PDF Download