As India completes 50 days of lockdown, this report presents the findings of a data-driven enquiry into the extent to which the lockdown has achieved its health objectives and arrested the spread of COVID-19. The success is measured on four parameters: flattening the curve, reducing the growth rate of new cases, containing the spread, and improving healthcare capacity. The findings show that while the lockdown has flattened the curve to an extent, it has failed to reverse the trend or contain the disease. Significant changes in strategy would have to be adopted to arrest the spread of COVID-19.
Attribution:
Sanjana Krishnan, Sahil Deo, Shardul Manurkar, “50 Days of Lockdown: Measuring India’s Success in Arresting COVID-19,” ORF Special Report No. 107, May 2020, Observer Research Foundation.
INTRODUCTION
On 24 March, when India went into a strict lockdown in response to the pandemic of COVID-19, there were only 519 confirmed cases across the country.[1]On 16 May, 53 days after the nationwide lockdown was imposed, India had 85,950 confirmed cases.[2]In this period, the country has gone through lockdown 1.0 (25 March to 14 April) lockdown 2.0 (15 March to 3 May), lockdown 3.0 (4 May to 17 May), and is in lockdown 4.0 from 18 May. So far, India has seen a ~165x increase in cases despite the extended periods of lockdown.
This report makes an assessment of the effectiveness of the lockdown in controlling the spread of the virus and determines the extent to which the lockdown has achieved its health objectives.
LOCKDOWN: AIMS vs. ACHIEVEMENTS
Objective 1: Flatten the curve to ensure that the number of cases that require hospitalisation stay below the capacity of the healthcare system, to minimise the number of preventable deaths
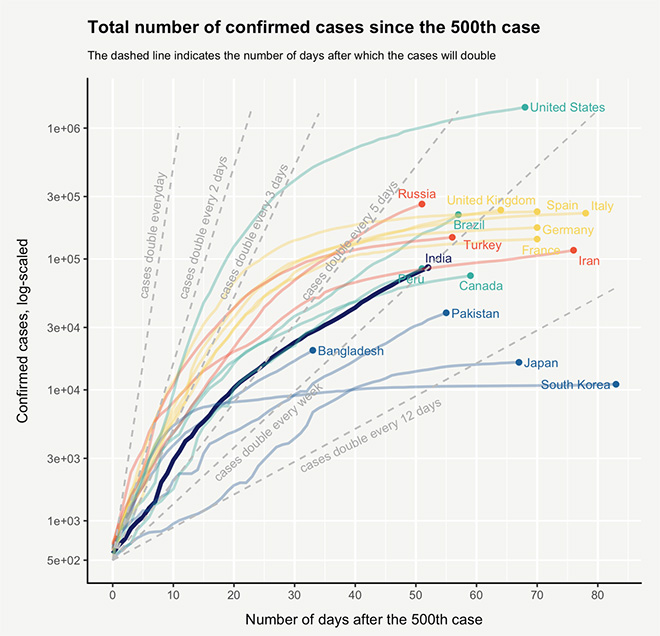
‘Flattening the curve’—a term which medical experts use in times of health emergencies—is the idea of slowing a virus’ spread so that fewer people need to seek treatment at any given time. The confirmed cases in India are growing at a rate of 5.56 percent and doubling roughly every 12.8 days.[3]In comparison to other countries, India has had a low doubling period because of the early enforcement of the lockdown, which helped reduce the nationwide doubling rate from the initial every five days to every ~13 days at the time of writing.[a]In contrast, ~50 days after the 500thcase, the US had 10 times more cases than in India. (See Figure 1)
Figure 1: Total number of confirmed cases in India compared to other countries
Graph shows the growth of total cases in countries after the 500thcase, the y-axis is log-scaled. The top 14 countries, Japan, South Korea, Bangladesh and Pakistan have been plotted. Dashed lines indicate number of days after which cases will double. Green colour: countries in Americas; yellow colour: Europe; blue colour: South and South-East Asia; Red: Central Asia and Russia. Source:Data compiled by Our World in Data (https://ourworldindata.org/covid-cases), data as of 16thMay 2020, analysis and visualisation by CPC Analytics
India has also managed to keep the number of cases below the capacity of the healthcare infrastructure in almost all districts. Less than 1.5 percent of the 130,000 hospital beds earmarked for positive cases in the COVID-19 wards are being utilised.[4]Mumbai is the exception, with news reports saying that a majority of the COVID-19 hospital beds are filling up.[5]Estimates on the number of people that would have been infected had there been no lockdown, with cases consistently doubling every three or seven days, show that the number of cases in India would have been 100 percent to 18200 percent higher, with a staggering 169,000 to 19,000,000 cases.[6]
If the rate of growth in the number of cases is the indicator, then the lockdown has worked, and the curve has been flattened to an extent. This has helped ease the burden on the healthcare system and in turn prevented thousands of potential deaths.
Objective 2: Reduce the number of new cases and turn the active cases line around
Before the lockdown can be lifted, in addition to reducing the growth rate of infections, the absolute number of daily new cases also needs to be reduced, especially when the absolute number of cases is high. This measure helps decision-makers assess the efficacy of containment by determining if the peak has been reached and the number of new cases are now in a downward trend (indicating a negative growth rate).
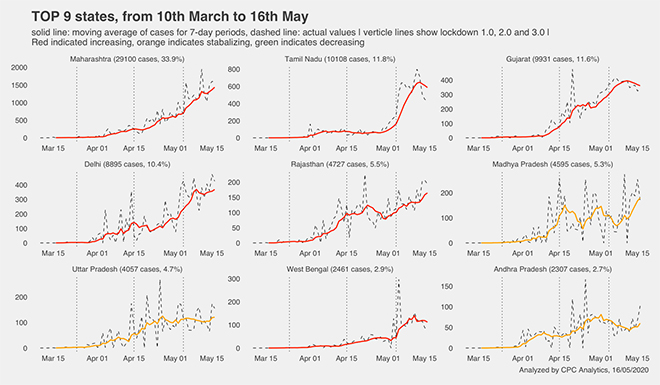
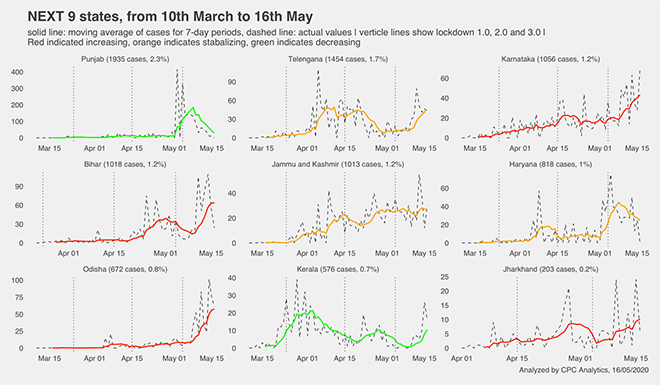
So far, there is no indication of the number of cases peaking (See Figure 2). Several small states like Himachal Pradesh and Uttarakhand, and a few big states like Kerala and Punjab are close to achieving the desired ‘inverted U’.[7]Similarly, several districts have made huge progress on this front, with Coimbatore, Palghar and Saharanpur showing good recovery, at least temporarily.[8]This trend provides hope for the several districts that have had a spike. As of 16 May, Andhra Pradesh, Haryana and Uttar Pradesh appear to have managed to stabilise the number of daily new cases.[9]
However, most of the big states are yet to peak in terms of number of new cases. Maharashtra, Gujarat, Tamil Nadu and West Bengal have all reported an increasing number of new cases every day despite the national lockdown.[10]
Another concerning trend is the emergence and rise of positive cases in several states after 3 May. The steep rise in Tamil Nadu, West Bengal, Bihar and Odisha in the last two weeks indicates that the problem has only begun for these states.
Figure 2: Cases in the top 18 states, from 10 March to 16 May
Dashed lines indicate the actual values, solid lines indicate the moving average for seven-day periods. Vertical lines show the start of lockdown 1.0, 2.0 and 3.0. Red indicates an increasing trend, orange indicates stabilisation and green indicates a decrease. Source:Data from the Ministry of Health and Family Welfare compiled, analysed and visualised by CPC Analytics. Data as of 16 May 2020.
Importantly, the growth of new cases is concentrated in a few districts even in these states, for instance, Mumbai, Ahmedabad, Chennai and Pune. Several other districts, especially in Bihar and Uttar Pradesh, have also registered a growing number of new cases, but the absolute numbers are relatively low.[11]Out of the 36 districts in Maharashtra, at least six are giving cause for concern while the situation appears to be stabilising in another six districts.[12]
If the number of daily new cases is the indicator, then the lockdown has had mixed results. While it has worked in some states and districts, most of the big states and several districts have failed to use the 50-day lockdown to turn the line around. In fact, even with the lower rate of growth, the absolute number of cases in this period has increased manifold.[13]This is because the rate of decrease has been extremely slow.
Objective 3: Containing the disease, preventing spread to newer districts and rural areas
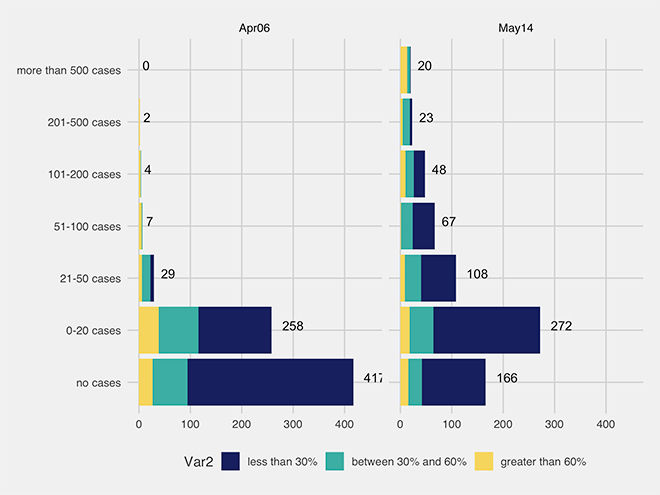
The distribution of cases in various districts on 6 April, two weeks after lockdown 1.0 started, and 14 May shows that there has been a huge shift in the profile of the districts affected. From being a primarily urban phenomenon two weeks after the lockdown began, the pandemic has spread to several new districts, including rural ones.
Figure 3: Districts divided by the number of cases and their level of urbanisation for 6 April (left) and 14 May (right). The graph shows the progression of COVID-19 in districts.
The two graphs show the number of cases in districts with urban population > 60%, between 30-60% and <30% at two snapshots of time (6thApril and 14thMay). The vertical axis shows case categories: no cases (bottom) to more than 500 cases (top). The length of the bar indicates the number of districts in each category.On April 6th, data was available for 717 districts. On May 14th, data was available for 706 districts. Delhi stopped reporting district-wise data for its 11 districts. Source:COVID cases- Government data compiled by How India Lives, analysed by CPC Analytics. Urban population data- Census 2011.
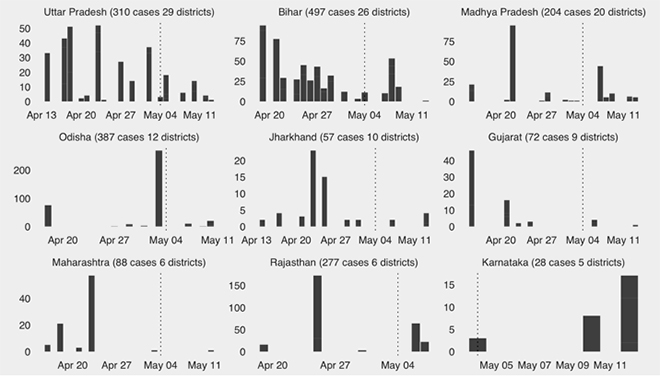
On 6 April, 417 districts had no cases. On 14 April (three weeks after the lockdown and at the start of lockdown 2.0), there were 324 districts with no confirmed cases. By 14 May, this number had fallen to 166 (See Figure 3). In effect, between 14 April and 14 May, 158 new districts reported cases. These include 29 districts in Uttar Pradesh, 26 in Bihar, 20 in Madhya Pradesh, and 12 districts in Odisha.
Figure 4: Spread of COVID-19 to green districts since lockdown 2.0
From 14 April to 14 May, 2712 positive cases were reported in 158 green districts. x-axis shows the date when the first case was diagnosed, y-axis shows the number of cases as on 14 May. Together, the nine states form 80.4 percent of all new cases post 14 April in districts that previously had no cases. Source:COVID cases- Government data compiled by How India Lives, analysed by CPC Analytics.
The late onset of the spread of the COVID-19 virus could be due to two reasons. The first could be late testing, particularly in Bihar and Uttar Pradesh, where only about 200 people per million were being tested at the end of April.[14]The second reason could be the exodus of migrants from hotspots to their homes in rural areas, primarily to the labour-producing states of Bihar, Uttar Pradesh, Madhya Pradesh, Orisha and Jharkhand. This would mean that there is a much wider community spread in the hotspots than previously anticipated.
So far, the numbers in the new districts are relatively low, but this trend needs to be closely observed in the coming weeks as more migrants move back.
It appears that inadequate testing and the inability of the central and state governments to provide migrants with adequate facilities and transportation to their hometowns early on, has resulted in the disease spreading to rural areas and a reduction in the number of green districts. This defeats one of the crucial objectives of the nationwide lockdown.
Objective 4: Use the lockdown to improve healthcare system’s capacity
To ensure that the lockdown is not being lifted prematurely, it is crucial to significantly ramp up the capacity of the healthcare system. If this is done, when the number of cases surge once the lockdown is lifted—which most experts believe will likely happen[15]—the healthcare system will be able to ensure that people do not die due to their inability to access medical services. The lockdown period helps pause the burden on the healthcare system and provides the government an opportunity to use the time to build the extra capacity needed for reopening. This is similar to the strategy adopted by Sweden, where the country has remained open because the number of patients in need for critical care is lower than the healthcare system’s capacity, and there is no need to recourse to triage.[16]
In India, the capacity has been stepped up in existing hospitals. At present, across the country, there are 970 COVID-19-only hospitals for critical patients, 2300 COVID-19 health centres for clinically moderate patients, and 645,000 (0.65 million) isolation beds for suspected cases and patients, some of which the government is trying to convert to hospital beds.[17]There are 130,000 hospital beds nationwide with ICU and oxygen facilities, and the current utilisation, as of 10 May, is only 1.5 percent. Officials also reported that there are more than 6,000 ventilators already available in dedicated COVID-19 hospitals and orders have been placed for 60,000 additional ventilators.[18]Cities like Mumbai are also building added facilities to meet the projected increase in hospitalisation.[19]
Health ministry data indicates that the severity of the disease across in India is low, with only 1.1 percent of all COVID-19 patients on ventilators, 3.3 percent on medical oxygen and 4.8 percent in ICU beds.[20]Rough estimates show that with a capacity of 6,000 ventilators, India can manage up to 545,500 cases without preventable deaths. With a capacity of 130,000 beds, the country can manage up to 1.4 million cases (provided the patients have access to medical oxygen and an ICU).[21]These numbers hold if the distribution of cases follows the distribution of the healthcare system’s capacity.
The lockdown has been partially used to improve capacity, but it is inadequate compared to the capacity that would be required if the lockdown were completely lifted. Also, it is important to ask if the government has been able to instill confidence in its citizens that once the lockdown lifts, and if the number of cases spike, those who fall ill will have access to health facilities and services.
WHAT NEXT?
The 50-day nationwide lockdown has so far slowed the growth in COVID-19 case numbers in most districts across India. However, it has been unable to pause or reverse the trend. The previously urban phenomenon has now spread to a larger geography. India is also facing the consequences of a lockdown that did not give enough thought to the realities of the country. The neglect of the healthcare system, inhumane and congested living conditions for the urban poor, and the lack of facilities for migrant workers in the cities have only made the control, containment and tracing of the disease more difficult. The effects of poor planning and implementation are showing, and it could be more pronounced in the coming weeks.
Fifty days after the lockdown, India is in an even more precarious condition than before (based on the four parameters outlined in this report). While the number of cases has stabilised in some districts, there are several others that previously had no cases but which have started to report some. To be sure, the situation could have been far worse. By merely slowing and not stopping the growth, however, India has reached a state like what it was on 24 March, albeit with more hotspots and a lot more cases. More data on testing, degree of contact tracing, healthcare capacity at the local level, and morbidity are needed to understand the true and full picture.
This has led the country to a catch-22 situation where it is forced to consider the tradeoff between lives and livelihoods, health and economy. However, India can still learn from its missteps and revamp its strategy.
One-size does not fit all, and there is an urgent need for local strategies tailored at the state, district, city, ward and containment zone level. This would ensure a better allocation of scarce resources to target the crisis. This would also allow decision-makers to lift the lockdown in areas that meet the criteria set by the World Health Organization (WHO).[22]The migrant inflow needs to be monitored by states. A drastic course-correction that keeps the poor at the heart of the decision-making is needed. Ramping up of healthcare facilities, especially in the hotspots, will prevent deaths, instill confidence and allow a return to normalcy as soon as possible.
India also needs a robust re-lockdown strategy, which is undoubtedly already in the works. Hopefully, lockdown 4.0 will provide the much-needed direction to deal with the crisis.
About the Authors
Sanjana Krishnan is a Partner, Sahil Deo is Co-Founder, and Shardul Manurkar is Lead of Legislative Research at CPC Analytics, a data-driven policy consulting firm with offices in Pune and Berlin.
[a]Considering an increase in cases in the two-week period as of 6 April and 16 May.
[21]. Calculations done by CPC Analytics based on availability of ventilators or beds and usage of ventilators or beds. For example, if there are 6000 ventilators available and 1.1% of COVID-19 patients require a ventilator, the 6000 ventilators can support 545,000 active cases (out of which 1.1% or 6000 patients would require ventilator) at any given point of time
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Sanjana is a partner at CPC Analytics. As part of CPC she has consulted for public sector and non-governmental organizations such as GIZ Swiss Agency ...
Non-resident fellow at ORF.
Sahil Deo is also the co-founder of CPC Analytics, a policy consultancy firm in Pune and Berlin. His key areas of interest ...
Shardul is the Lead (Legislative Research) at CPC Analytics. As part of CPC he produces legislative briefs bill summaries and issue briefs for elected representatives ...

 PDF Download
PDF Download