
-
CENTRES
Progammes & Centres
Location
As many countries in the Indo-Pacific struggle to meet their vaccination targets, India could spearhead a vaccine initiative in close collaboration with other players to ensure vaccine equity in the region

This piece is part of the series, Sustainable Development in the Indo-Pacific
As the year 2021 was coming to an end, many hoped that the COVID-19 pandemic would show signs of dying down in most parts of the world. The virus circulation was lower and most countries were learning to “live” with the SARS- CoV-2 virus. In India, the festive season was making authorities apprehensive as they were expecting a rise in cases. At around the same time, health agencies in South Africa detected a new strain, Omicron, which has now spread to most of the world and is causing the next wave of COVID-19. Throughout the course of the pandemic, the World Health Organisation (WHO) has called for countries to come together and fight as one. The Indo-Pacific can play an important role in setting an example to this effect. Such a collaboration between the Indo-Pacific countries can also catapult India to the forefront of this geopolitical region.
The Quad—a group of like-minded democracies comprising India, Japan, Australia and the United States (US)—is seen to be one of the foremost groupings in the Indo-Pacific region. The genesis of the Quad lies in 2004 when India, the US, Australia, and Japan coordinated relief during the deadly Indian Ocean tsunami. India, however, views the Indo-Pacific as inclusive of all countries that lie within this geographical area. The initial collaborations since then have mainly centered on marine ecosystems, security and trade. Healthcare is a recent addition to these avenues of collaborations. To contain the pandemic, the Quad leaders have pledged to work closely for better response to exigencies arising due to COVID-19. More than 1 billion vaccines will be donated globally by the Quad. As of 25 September 2021, a total of 79 million vaccines had been donated to other countries in the Indo-Pacific. Other related areas such as manufacturing and supply chain management of vaccines are also identified for close collaboration amongst the Indo-Pacific countries.
The Quad leaders need to include vaccine equity—both inter and intra nation—in their healthcare mandate for the Indo-Pacific region. Recent data highlights that amongst global low-income countries, only 4.2 percent of the total population is fully vaccinated. Population vaccination proportions for middle- and high- income countries were a median 35 percent and 70 percent, respectively. One reason for the median difference was reported to be ‘delayed authorisation’ for vaccine use in lower-middle-income countries where clinical trials were conducted.
The framework of COVAX is not sufficient, and the Indo-Pacific can collaborate more closely to ensure vaccine equity.
For India, the Oxford Astra-Zeneca Covishield was the first vaccine to begin Phase 2 and 3 clinical trials. Manufactured locally by the Serum Institute of India, the trials only began from August 2020, i.e., three months after the biological viral material was first obtained from Oxford University in May 2020. It took five months subsequently for Covishield to be administered to Indians starting from 16 January 2021. The rollout for Covaxin, an indigenous COVID-19 vaccine and the second vaccination approved in India, also had a similar timeline for approval and use in India. For Covishield, although manufactured locally, vaccine doses were prioritised for countries that were classified as high- or middle-income. Countries were already finding ways of reserving vaccines even before the vaccine was developed. Bilateral or multilateral agreements between countries were already in place. Many resorted to the method of direct procurement from manufacturers/companies, who are mostly based in middle- or high-income countries.
COVAX (COVID-19 Vaccines Global Access) was established by the WHO to ensure vaccine access for every country. It is, however, not proving to be successful at achieving the aim it was set up for. Low- or low-to-middle-income countries are still at a disadvantage when it comes to equitable access to the vaccine. High-income countries had purchased doses for as early as May 2020, even before the vaccine companies began any human trials. For COVAX to deliver on its commitments, a sort of vaccine refund or vaccine return will need to be carried out by countries who purchased in advance. With Omicron now gripping the world, there is no chance of this happening.
Although the COVAX’s mechanism of fair allocation of vaccines highlights on prioritising vaccine access to those nations where threat and ‘vulnerability’ to COVID-19 is high but every nation, in one way or the other, is at threat from or is vulnerable to COVID-19. Even previously, when India took the onus and sent a million doses to the US, who were reeling under the third wave, India’s decision was heavily criticised by political parties closer home as months later India was hit by the second COVID-19 wave. Driven by the Delta variant, India witnessed daily surges in cases, hospitalisations, and deaths. The criticism was sharp and it questioned the Indian government’s ‘charity’ to other countries—whose threat and vulnerability were higher—while choosing not to first vaccinate its own citizens. The mandate to work towards vaccine equity reduces under this light. This has been the case for when other nations world over were struck by the second, third, or fourth wave of the pandemic. High-income countries like the US halted the export of raw materials for vaccine manufacturing to India as they prioritised preparing themselves against the Delta variant.
Although the COVAX’s mechanism of fair allocation of vaccines highlights on prioritising vaccine access to those nations where threat and ‘vulnerability’ to COVID-19 is high but every nation, in one way or the other, is at threat from or is vulnerable to COVID-19.
Looking inwards, according to the World Bank, the Indo-Pacific region is home to more than half a dozen countries that are classified as low-income and low-middle income. These low- and low-middle-income countries also account for a higher population share in the region. As of 1 January 2022, Singapore had the highest vaccination rates in the Indo-Pacific.
Figure 1: Percent proportions of COVID-19 vaccinated population as of 5 January 2022
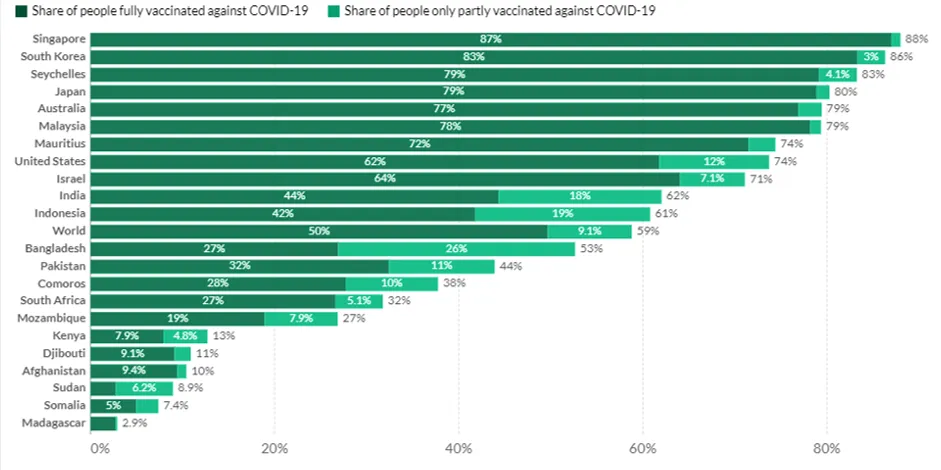 Source: Ourworldindata.org
Source: Ourworldindata.org
The evidence points to vaccine coverage being differential according to a country’s income classification. For high-, middle- and low-income countries, there are 58.49, 11.95, and 1.26 doses/100 population count, respectively. Vaccination policies are stronger in high-income countries whereas low-income countries have weaker and limited policies. These policies were also found to mediate vaccination coverage. The framework of COVAX is not sufficient, and the Indo-Pacific can collaborate more closely to ensure vaccine equity. India’s absolute numbers of vaccinations are impressive and surpass all others in the Indo-Pacific. While there is much to learn for other countries on this front, there is, however, the underlying concern that a large part of the population is still unvaccinated, and urban-rural divide for COVID-19 vaccinations remains as well. Countries in the Indo-Pacific who have higher rates of vaccinations need to support existing efforts for other low- and middle-income countries to achieve the WHO-set target of 70 percent population being vaccinated by July 2022 to contain the pandemic.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Dr. Ekta Jain has more than 13 years of experience in bioinformatics epidemiology data analytics databases andcomputer programming. She was a recipient of the National ...
Read More +


