
-
CENTRES
Progammes & Centres
Location
The central challenge in DAMH is the misalignment between the goals of recipients and the priorities of donors

Mental health is a basic human right and an integral part of health and well-being, determined by a myriad of individual, structural and social determinants, such as heredity, exposure to war, and environmental degradation, among others. However, it continues to be one of the most neglected areas of public health, marked by underinvestment and stigma, especially in low- and middle-income countries. Fragmented mental health services, insufficient human resources, discrimination, and a lack of government support often contribute to this neglect. International assistance and cooperation, therefore, is necessary to address this issue by sharing knowledge and implementing effective strategies for detection, prevention, and treatment.
Development assistance for mental health (DAMH) is a crucial means of providing necessary resources and support to low- and middle-income countries.
Development assistance for mental health (DAMH) is a crucial means of providing necessary resources and support to low- and middle-income countries. To trace funding flows of mental health assistance (MHA), we analysed data from the Development Assistance for Health Database by the Institute of Health Metrics and Evaluation (IHME). This study presents a snapshot of MHA from 2000-2021, and examines changes during the COVID-19 pandemic. While MHA may be provided under various sectors, from education, infrastructure, to health, we look at MHA under health in this article in order to juxtapose it with its increasing share to Disability Adjusted Life Years (DALYs).
MHA constituted only 0.27 percent of the total health assistance provided by donors, and less than 1.2 percent of assistance given by any country from 2000-21. There was a sudden spurt in MHA in 2018, and it then plummeted in 2020.
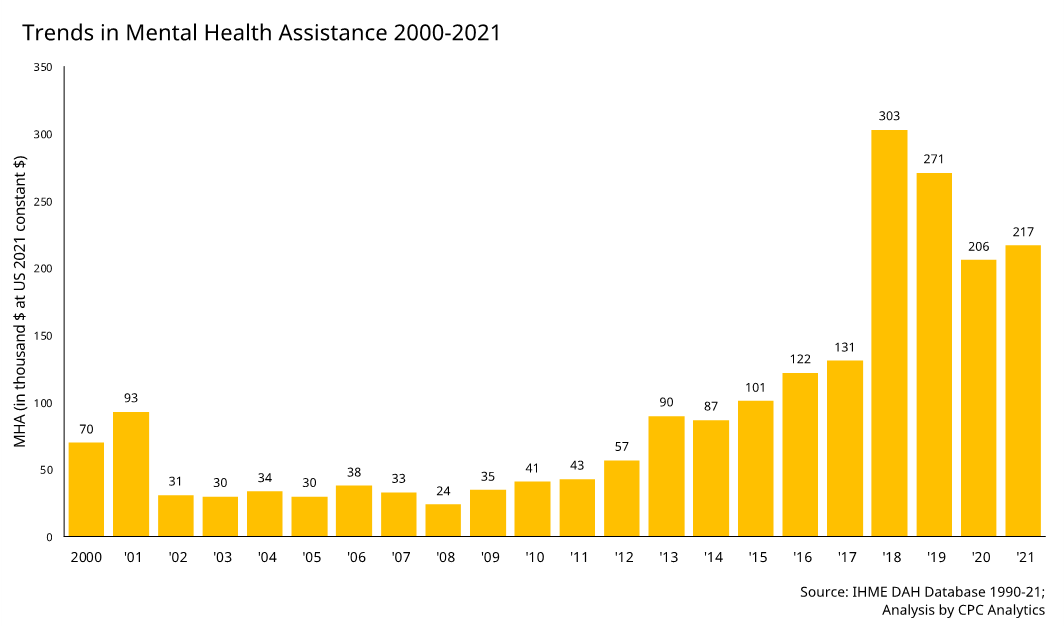
This fall could be attributed to diversion of funds to COVID-19, as is evident by the sudden spurt in assistance allocated under the category of ‘Other infectious diseases’ in the IHME DAH database (30.7 percent of all assistance in 2020, as against 6.7 percent in 2019). However, when compared to funding patterns in other health focus areas such as HIV/AIDS, neonatal and child health, reproductive and maternal health, which reduced drastically during the pandemic, the level of funding of mental health assistance has remained constant at 0.3 percent.
We identified 30 donors for MHA since 2000. Twenty six of them are countries, and four are non-state actors, which include the Bill and Melinda Gates Foundation and three others comprising corporate donations, private funding, and others. The countries contributed to 46 percent of the total MHA, whereas other entities, corporate, private funding, and others contributed to 54 percent of the total share. All the donor countries were high income countries, except China, which is an upper middle-income country. Since 2000, the greatest contribution to MHA has been private sector financial contributions by corporations, foundations and individuals (45.8 percent), followed by the United States (9.2 percent) and United Kingdom (8.5 percent), indicating the increasing share of private entities and means (such as philanthropes) in the mental health development sector.
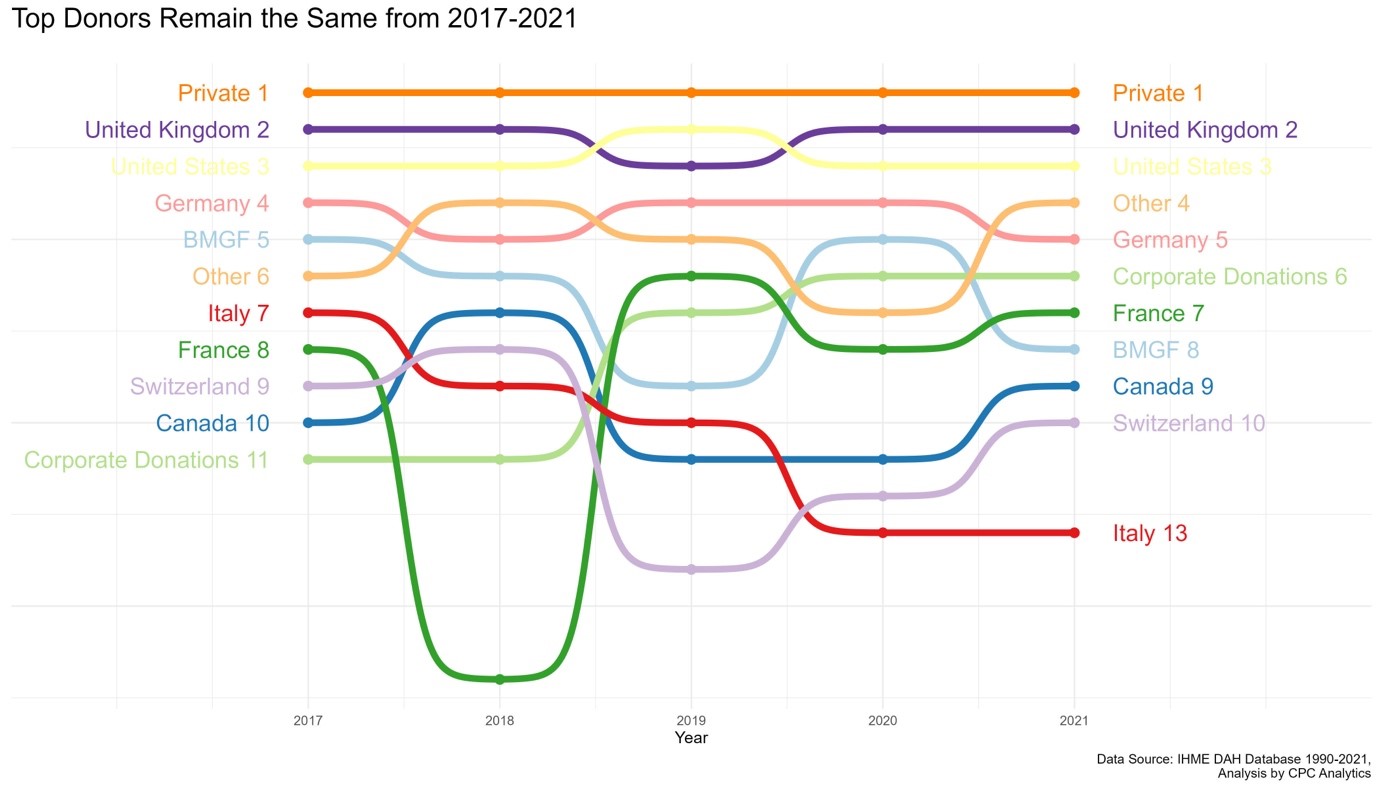
The chart above explores the changes in rankings of the top donors in MHA from 2017-21. Private donors have constituted the highest share in donorship since 2017[1]. Based on limited data available, it is difficult to ascertain what aspects of mental health are precisely funded through mental health assistance. According to WHO Mental Health Atlas 2017, majority of DAMH is directed towards training workforce, awareness programmes, and other community-based interventions and services. It also varies according to countries. In India, for example, corporate organisations and private funding in MH is often done in areas of rehabilitation, awareness building, and scholarships to academicians to pursue their careers in the field.
From 2000-21, approximately 83 percent of MHA had gone to unspecified/unallocated regions or in administrative expenses, and 17.1 percent went directly countries. In 2021, all of MHA went to unallocated/unspecified regions. Given that the biggest chunk of MHA is categorised under unallocated/unspecified recipients or is expended as administrative expenses, we looked at the channels of these funding to understand its flow.
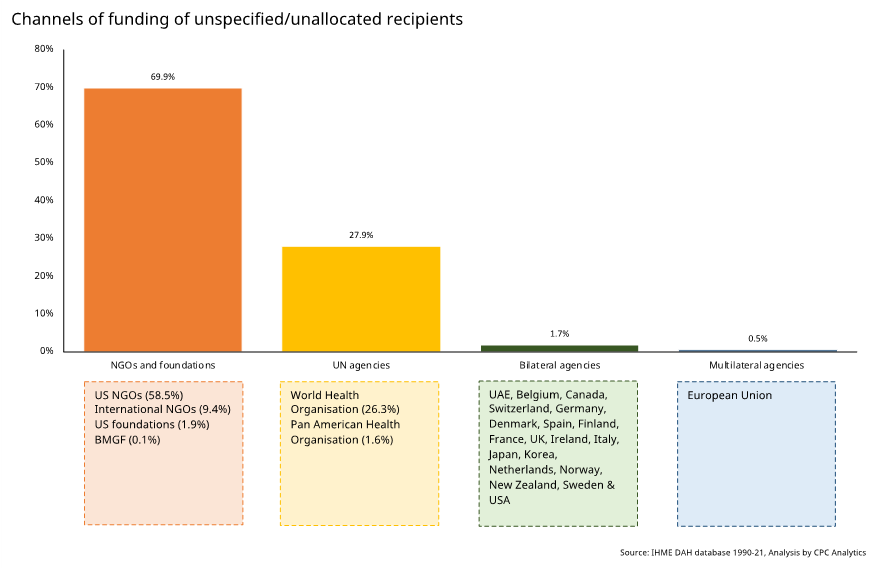
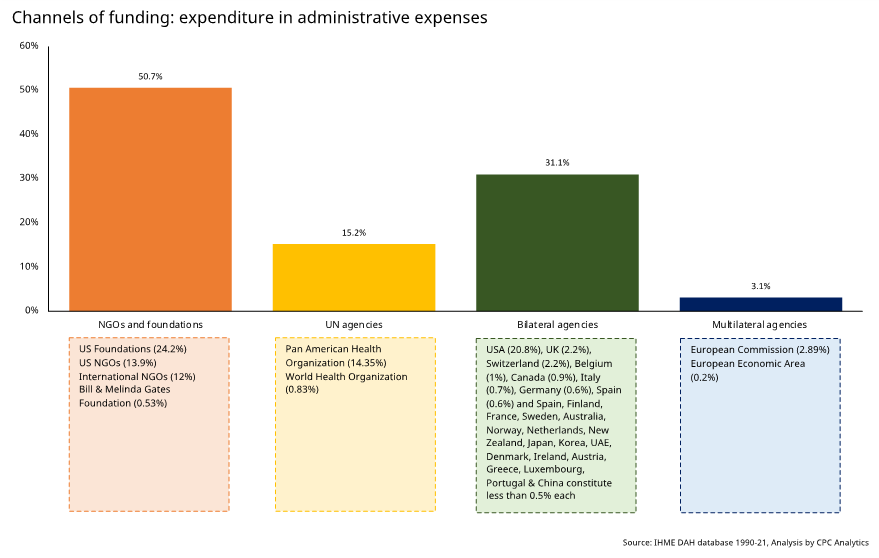
In both unallocated/unspecified and administrative expenditures, a majority of aid is channelled through NGOs and foundations, particularly from the United States and international NGOs and United Nations agencies such as World Health Organisation and Pan American Health Organisation. Bilateral agencies of donor countries also contribute significantly towards assistance characterised as unallocated/unspecified and administrative expenses.
Existing literature on funding patterns in health assistance notes that donor countries provide development assistance for health and mental health depending upon a wide range of factors, such as aid provided previously, income level of country (GDP per capita), conflict and natural disasters, trade relations of the donor and recipient country and government health expenditure.
Disability-adjusted life year is a measure of overall disease burden, expressed as the number of years lost due to ill-health, disability or early death.
While there are many ways to conduct analysis of why some countries get more aid than others, we use the health metric of Disability Adjusted Life Years of mental health. Disability-adjusted life year is a measure of overall disease burden, expressed as the number of years lost due to ill-health, disability or early death. It helps understand how diseases and medical conditions affect the length and quality of life for a given population. DALYs of mental health indicate the burden of mental disorders of a country[2]. Since the most recently available data of DALY for mental health is of 2019, we compare the average mental health assistance received by all recipients (exclusive of unallocated/unspecified, administrative expenses and global) with their respective DALY of mental health for 2019, to understand the correlation between the burden of mental health diseases and assistance provided to countries.
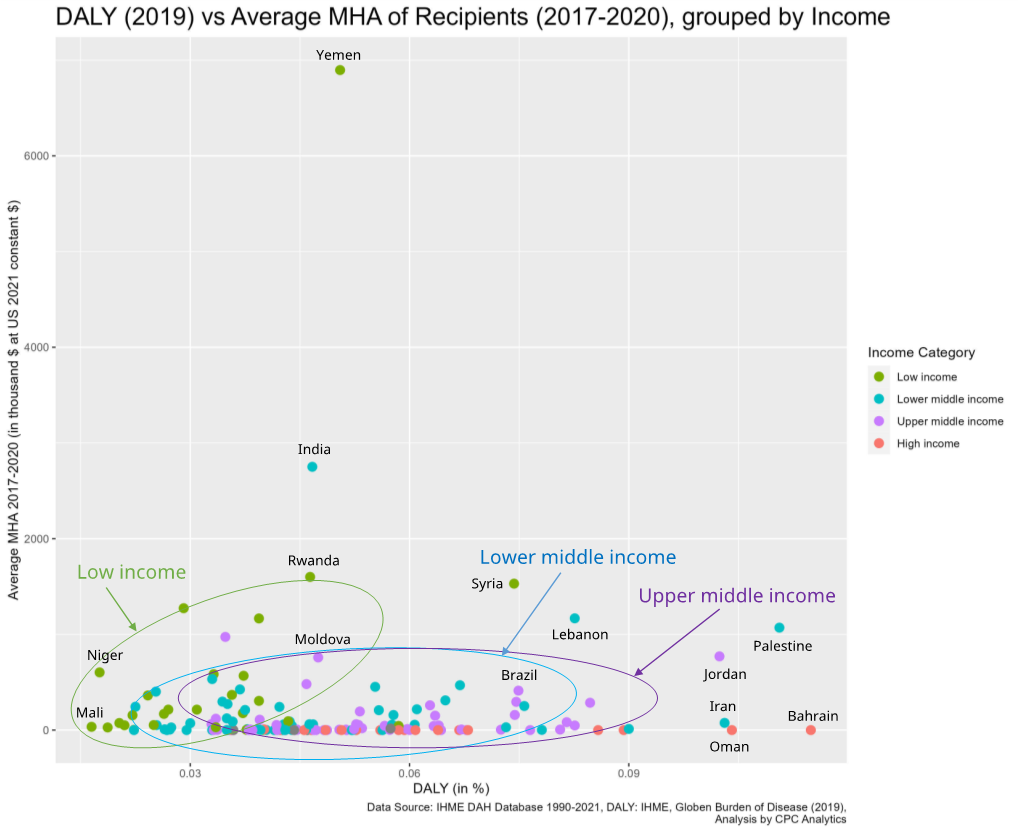
The graph compares the average mental health assistance of recipient countries from 2017-20 and compares it with the DALY due to mental disorders and conditions of 2019. Upper middle income countries, which usually report higher DALYs, have received no or very little mental health assistance. This is veritably so, since upper middle income countries are expected to have the resources to cover up for their health expenditure. However, it is worthwhile to note that these upper middle countries are receiving health assistance for other health focus areas, such as HIV/AIDS, health systems strengthening, child and neonatal health etc.
Lower middle income countries tend to be concentrated in the middle, with higher DALYs than low income but lower than upper middle income countries. Lower middle income countries with high DALYs (such as Palestine, Iran and Lebanon) receive relatively higher amounts of mental health assistance.
Upper middle income countries, which usually report higher DALYs, have received no or very little mental health assistance.
Low income countries tend to report lower DALYs, due to inadequate infrastructure for mental health care, or low levels of reporting. However, the graph shows that as DALYs increase, the MHA given to low income countries also increases.
In general, MHA was given to low middle income countries (6.6 percent), followed by low income (5.8 percent) and upper middle income (4.4 percent) countries. Some of the highest recipients have been Palestine, Yemen, India and Rwanda.
A more granular analysis into the recent years is warranted to see the latest trends in MHA. The table below highlights the changes in top recipients of mental health assistance from 2017 to 21 of top 10 recipient countries of each year.
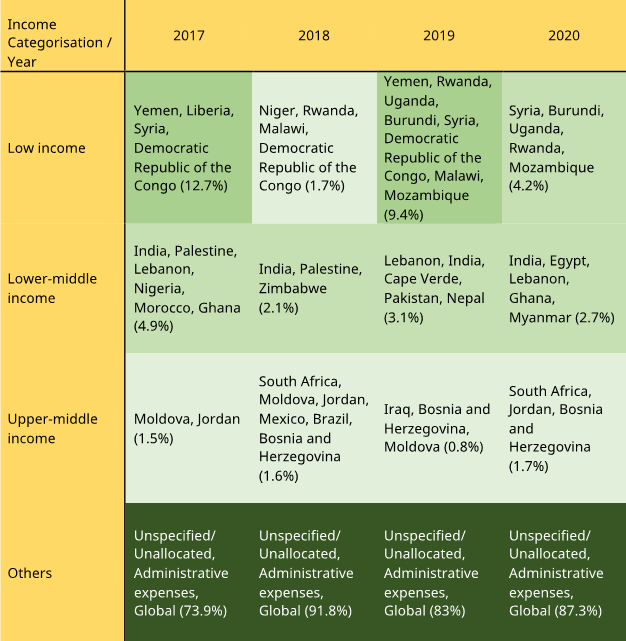
Source: IHME DAH Database 1990-21; Darker gradient of green shows higher share of mental health assistance
In the recent years, the share of lower middle income countries as recipients of MHA has reduced. This stands in contrast to the trends seen in 2000-21, where lower middle income countries constituted a greater proportion of MHA than low middle income countries.
This research details patterns of funding of MHA from 2000-21.
Existing literature notes that the central challenge in DAMH is the misalignment between the goals of recipients and the priorities of donors. Mental health conditions require tailored techniques for diagnosis and treatment, which are often not taken into account when allocating funding and resources. In addition, many recipient countries lack the necessary tools and expertise to effectively utilise advanced technologies or provide adequate human resources and infrastructure to promote and treat mental health conditions. Improving DAMH requires both structural and operational changes. The flow of aid needs to be well-directed and transparent, and it is important to establish monitoring tools and ensure accountability for the money spent. Low- and middle-income countries, as well as those in conflict, are the ones that require the most aid in the mental health sector. Given their shared history and similar levels of economic and human development, increased coordination and cooperation among them is needed. To stimulate dedicated donor flows, it is essential to re-evaluate the need and status of DAMH with innovative and objective methods formulated to measure the need, flow, and impact of the funds.
Sahil Deo is co-founder of CPC Analytics
Christian Franz is co-founder of CPC Analytics
Rajat Khosla is the Director of the United Nations University International Institute for Global Health (UNU-IIGH).
The authors would like to thank Ovee Karwa, Jayati Sharma and Shambhavi Joshi for their contributions to this research.
[1] Private donors are separate from corporate donations, which are specifically in-kind contributions to NGOs. ‘Other’ constitute interest, transfer of funds, refunds, miscellaneous income earned by channel of funding.
[2] DALYs include Depression, Bipolar Personality Disorders, Anxiety, Schizophrenia, Intellectual Disabilities, Conduct Disorders, Autism Spectrum Disorders, Eating Disorders, Attention Deficit or Hyperactivity Disorders among others.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Non-resident fellow at ORF. Sahil Deo is also the co-founder of CPC Analytics, a policy consultancy firm in Pune and Berlin. His key areas of interest ...
Read More +
Christian Franz are co-founders of CPC Analytics a data-driven policy consulting firm with offices in Pune and Berlin. ...
Read More +
Rajat Khosla is a Director, United Nations University, International Institute on Global Health ...
Read More +


