
-
CENTRES
Progammes & Centres
Location
India will need to invest in a resilient information infrastructure, and 2021 would hopefully see relevant and scientific information being a catalyst in initiatives within the healthcare delivery system. The COVID-19 vaccination drive will be a testing ground.

This article is part of the series — India and the World in 2021.
It would not be an overreach to say that India’s health policy is taking centrestage in public discourse largely because of the COVID-19 pandemic; otherwise, it has been a neglected area of state intervention in the country, as far back as after independence. To be sure, there have been efforts to undo the decades of neglect as policymakers began to acknowledge that the global Sustainable Development Goals (SDGs) — to which healthcare is fundamental — cannot be achieved if India fails to meet them. It is also true that if India indeed succeeds, with all its continent-sized problems, an “India Model” can serve as a blueprint for large parts of the world to emulate. While this is true for most social sectors, it is especially relevant for health, where globally recognised bottlenecks that limit the population’s access to healthcare services are scaled to the extreme.
Over the past decades, India’s health outcome indicators have shown slow but consistent improvement; much of these achievements were met despite inadequacies in both policy attention and funding. When the National Health Policy 2017 set a target of reaching 2.5 percent of GDP worth of government expenditure in health by 2025, most analysts were of the view that it was highly ambitious. India indeed appeared to be far from able to achieve such target (See Graph). However, the global COVID-19 pandemic in 2020 forced the Government of India to spend way beyond its own 2025 target, and in many ways, above its means.
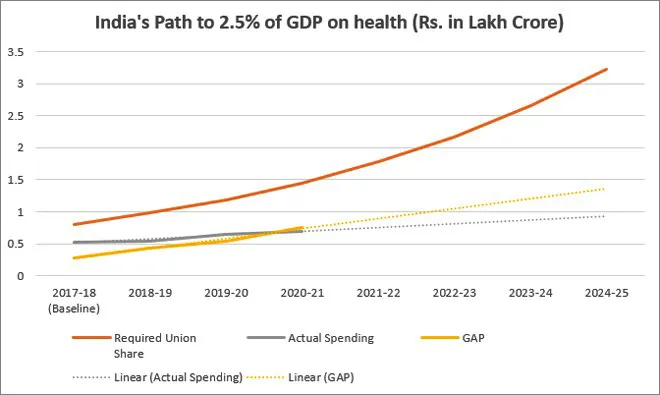 Source: Fifteenth Finance Commission and Budget Documents
Source: Fifteenth Finance Commission and Budget DocumentsBy the middle of 2020, it was clear that COVID-19 will prove to be a slow-moving national crisis, spilling over to the next year or two. To make things worse, data from years preceding the pandemic had already showed a slowdown and even reversals in infant and child mortality decline in large parts of India, particularly in urban areas. Thus, the pandemic has amplified existing problems within India’s health system — including a crisis of malnutrition — and the country faces even more massive challenges in 2021.
Given this context of a long-drawn pandemic response, freeing up sufficient resources — financial and otherwise — for the treatment of non-COVID-19 conditions is going to be the primary challenge in 2021. By some estimates, India’s gross domestic product has contracted by 10·3 percent, and the economy is not expected to be back on track soon. This would mean that new sources will need to be tapped for sustained, extra funding for the healthcare sector. The Fifteenth Finance Commission had projected a ₹5.38-lakh crore requirement for the Ministry of Health between 2020 and 2025 for providing primary healthcare, and the widely expanded requirements of immunisation, screening, testing and treatment of COVID-19 may result in an upward revision. The imperative for an almost parallel structure to treat non-COVID-19 conditions will see this amount growing many times over.
In turn, optimal utilisation of limited resources in the health system would necessitate effective knowledge- and information-sharing. As the pandemic broke out across India, risk communication quickly emerged as the weakest link in the country’s healthcare ecosystem. Along with healthcare services, India’s Health Management Information System (HMIS) itself was severely disrupted by the pandemic, and incomplete information resulted in the proliferation of faulty analyses and conclusions that did not inspire confidence but instead induced panic. India will need to invest in a resilient information infrastructure, and 2021 would hopefully see relevant and scientific information being a catalyst in initiatives within the healthcare delivery system. The COVID-19 vaccination drive will be a testing ground.
Facilitating cross-learning between states, and curation of best practices remains an area where some initial steps have been taken; but much more needs to be done. The pandemic will possibly push an estimated 400 million people deeper into poverty in 2021, and this will require a cooperative federal system handling health response as a joint responsibility of the central, state, and local governments and the citizens. Health still happens to be a State Subject in India’s federal system and the High Level Group on Health constituted under the Fifteenth Finance Commission recently recommended the shifting of healthcare to a Concurrent Subject.
Maintaining and accelerating the progress made towards Universal Health Coverage will require innovation from the village levels, up. After all, structural weaknesses within India’s healthcare delivery system have been exposed by the pandemic, ranging from “inadequate medical supplies and insufficient numbers of health-care workers in public hospitals to irrational treatments and profiteering by private hospitals.” Ensuring the equitable distribution of vaccines, medicines, diagnostics and healthcare workforce would therefore require the Centre and States to intervene with an equal sense of ownership, even as the private sector and civil society are encouraged to become constructive participants.
A study has estimated that India needs 2.07 million doctors by 2030 if it is to provide equitable healthcare. Aware of this exigency, the Government of India is expanding medical seats, both at the public and private sectors, with an aim of filling rural gaps. According to latest available estimates, the number of MBBS seats has seen a jump of 48 percent, from 54,348 in 2014-15 to 80,312 in 2019-20. There has also been a 47-percent increase in the number of government medical colleges during the period between 2014 and 2019, compared to a significantly lower 33-percent increase in the total number of medical colleges — including government and private — in the past five years, from 404 in 2014-15 to 539 in 2019.
Inadequacies in health facilities are often exacerbated by structural inequalities drawn by class, caste, gender, geography, and religion; they require solutions that adapt to local realities. For these reasons, leveraging digital innovations to improve access in India will have to run parallel to initiatives aiming to bridge the digital divide across the country’s socio-economic gradients. India’s strengths as a digital powerhouse have yet to be harnessed by the health system to accelerate its progress towards a high-quality, affordable, comprehensive, accountable, accessible and inclusive healthcare for all. The National Digital Health Mission will have a creative role towards building a healthcare ecosystem with these characteristics, if a consultative and participatory engagement is followed with the diverse stakeholders.
2021 could also be the year when India consolidates and expands on its social determinants of health (SDH) approach. Over the last decade, the Indian state has been silently working on translating the SDH framework into practice, with key interventions in the areas of nutrition (National Nutrition Mission), drinking water (Har Ghar Jal), indoor air pollution (Ujjwala Yojna), sanitation (Swachh Bharat), road access (Gram Sadak Yojana), and gender (Beti Bachao Beti Padhao).
It is a truism that every crisis also presents an opportunity. For India, if the current interest in strategic health policy as a key pillar of the economy is sustained — then the pandemic can be said to have played its part in history.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Oommen C. Kurian is Senior Fellow and Head of Health Initiative at ORF. He studies Indias health sector reforms within the broad context of the ...
Read More +


