
-
CENTRES
Progammes & Centres
Location
Successful stories of change across India suggest investment in girls and women and heightened delivery of health and nutrition interventions in bringing down malnutrition.
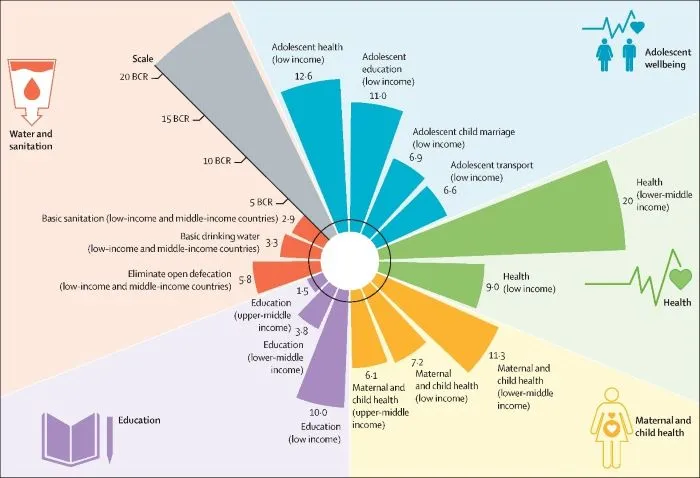
 Breaking the Intergenerational Cycle of Undernutrition is one of the key pillars towards eliminating malnutrition from the country. For India, breaking the Intergenerational Cycle of Undernutrition has seen a history of neglect. Intergenerational influences are defined as “conditions, exposures, and environments experienced by one generation relate to the health, growth and development of the next generation.” Significant incidence of early marriage and childbearing are amongst the important causes of undernutrition, due to the adverse intergenerational bearing on health, education and employment. Investment in maternal and child health, and adolescent well-being, (Figure 1) yields a high cost to benefit ratio, with a triple dividend in both low and upper-middle income countries.
Figure 1: Benefit Cost Ratio-return on every dollar invested
Breaking the Intergenerational Cycle of Undernutrition is one of the key pillars towards eliminating malnutrition from the country. For India, breaking the Intergenerational Cycle of Undernutrition has seen a history of neglect. Intergenerational influences are defined as “conditions, exposures, and environments experienced by one generation relate to the health, growth and development of the next generation.” Significant incidence of early marriage and childbearing are amongst the important causes of undernutrition, due to the adverse intergenerational bearing on health, education and employment. Investment in maternal and child health, and adolescent well-being, (Figure 1) yields a high cost to benefit ratio, with a triple dividend in both low and upper-middle income countries.
Figure 1: Benefit Cost Ratio-return on every dollar invested
 Source: The Lancet
Source: The Lancet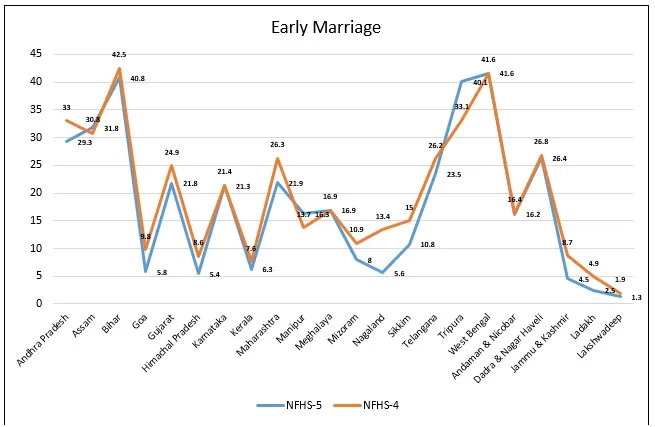 Figure 3: Trends in teenage pregnancies in the 22 states/UTs
Figure 3: Trends in teenage pregnancies in the 22 states/UTs
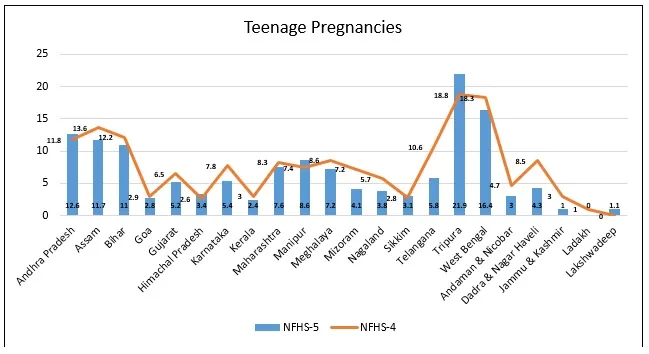 Of concern is Tripura, showing a steep incline in both child marriage and teenage pregnancies. Assam and Manipur also show a rise in child marriage. Other than Tripura, Andhra Pradesh, Himachal Pradesh, Manipur, Sikkim and Lakshadweep a show rise in teenage pregnancies. Lakshadweep, at 1.1 percent teenage pregnancies, has risen from zero percent since the last survey prior to the NFHS-5 (2015-16).
Malnutrition trends are alarming, with eleven states show a rise in stunting in children under five; the highest being reported from Meghalaya (46.5%), and Bihar (42.9%). The NFHS-5 shows a sharp rise in stunting for Kerala, Goa and Tripura, which is a cause for concern. Wasting remains stagnant or shows a rise in most of the states/UTs. Underweight population is on the rise in 11 states. The threat of double burden of malnutrition <1> is evident from the increasing trend in overweight prevalence in children under five. A steep incline in overweight children under five has been observed in the states of Himachal Pradesh and Mizoram, and the union territories of Ladakh and Lakshadweep. The data on nutritional status of women on the one hand indicates a decline in percentage of women who are thin (BMI less than 18.5), and a sharp incline in women who are obese/overweight in 16 of the 22 states/UTs.
Evidence indicates that children born to adolescent mothers have a 10 percent higher prevalence for stunting. Case studies from across India show how adolescents and young girls get consumed into the intergenerational cycle of malnutrition. The Intergenerational Cycle of Undernutrition is heightened by poverty, social exclusion and gender discrimination, leading to irreversible effects on cognitive and physical development. The intergenerational cycle of malnutrition can be combatted through robust interventions for both mother (pre- and post-pregnancy) and child, thereby, addressing the high burden of stunting.
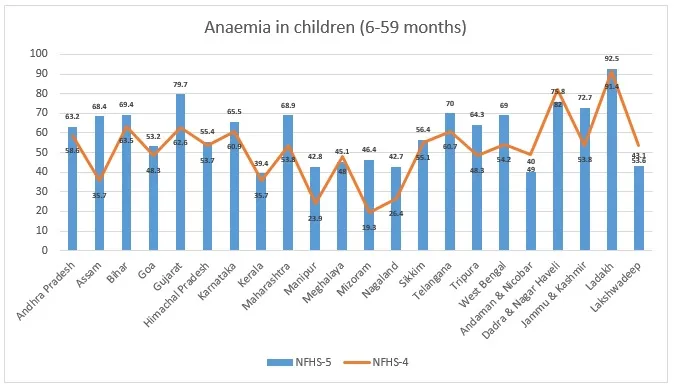
Figures 4, 5 and 6 indicate the anaemia trend in children under five, women (15-49 years) and adolescent girls (15-19 years). It is a clear indication of the rise of anaemia in both children and women. Anaemia in children under five has increased in 16 states/UTs, with a very significant rise in the states of Assam (32.7 percentage points), Mizoram (27.1 percentage points), Manipur (18.9 percentage points), and UT of Jammu and Kashmir (18.9 percentage points,) to name a few.
Figure 4: Anaemia prevalence in children under-five years in the 22 states/UTs
Of concern is Tripura, showing a steep incline in both child marriage and teenage pregnancies. Assam and Manipur also show a rise in child marriage. Other than Tripura, Andhra Pradesh, Himachal Pradesh, Manipur, Sikkim and Lakshadweep a show rise in teenage pregnancies. Lakshadweep, at 1.1 percent teenage pregnancies, has risen from zero percent since the last survey prior to the NFHS-5 (2015-16).
Malnutrition trends are alarming, with eleven states show a rise in stunting in children under five; the highest being reported from Meghalaya (46.5%), and Bihar (42.9%). The NFHS-5 shows a sharp rise in stunting for Kerala, Goa and Tripura, which is a cause for concern. Wasting remains stagnant or shows a rise in most of the states/UTs. Underweight population is on the rise in 11 states. The threat of double burden of malnutrition <1> is evident from the increasing trend in overweight prevalence in children under five. A steep incline in overweight children under five has been observed in the states of Himachal Pradesh and Mizoram, and the union territories of Ladakh and Lakshadweep. The data on nutritional status of women on the one hand indicates a decline in percentage of women who are thin (BMI less than 18.5), and a sharp incline in women who are obese/overweight in 16 of the 22 states/UTs.
Evidence indicates that children born to adolescent mothers have a 10 percent higher prevalence for stunting. Case studies from across India show how adolescents and young girls get consumed into the intergenerational cycle of malnutrition. The Intergenerational Cycle of Undernutrition is heightened by poverty, social exclusion and gender discrimination, leading to irreversible effects on cognitive and physical development. The intergenerational cycle of malnutrition can be combatted through robust interventions for both mother (pre- and post-pregnancy) and child, thereby, addressing the high burden of stunting.
Figures 4, 5 and 6 indicate the anaemia trend in children under five, women (15-49 years) and adolescent girls (15-19 years). It is a clear indication of the rise of anaemia in both children and women. Anaemia in children under five has increased in 16 states/UTs, with a very significant rise in the states of Assam (32.7 percentage points), Mizoram (27.1 percentage points), Manipur (18.9 percentage points), and UT of Jammu and Kashmir (18.9 percentage points,) to name a few.
Figure 4: Anaemia prevalence in children under-five years in the 22 states/UTs
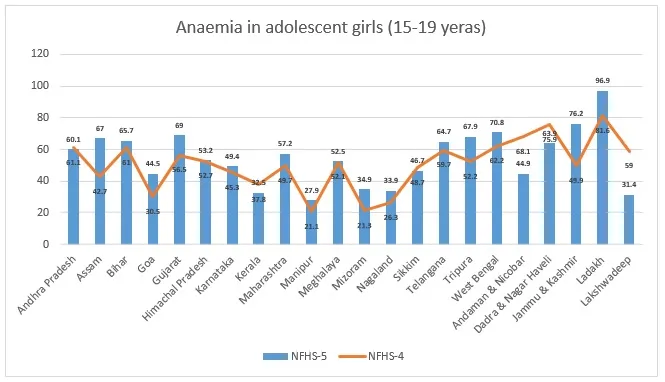
 Anaemia in women of reproductive age (15-49 years) shows an incline in 16 states/UTs. Assam (19 percentage points), Jammu and Kashmir (17 percentage points), and Ladakh (14.4 percentage points) show the highest incline in anaemia levels. Looking at trends for anaemia in adolescent girls (15-19 years), again 16 states/UTs show an incline. A sharp rise can be observed in Jammu and Kashmir (26.3 percentage points), Assam (24.3 percentage points), Tripura and Ladakh with 15.7 and 15.3 percentage points respectively.
Figure 5: Anaemia prevalence in women of reproductive age (15-49 years) in the 22 states/UTs
Anaemia in women of reproductive age (15-49 years) shows an incline in 16 states/UTs. Assam (19 percentage points), Jammu and Kashmir (17 percentage points), and Ladakh (14.4 percentage points) show the highest incline in anaemia levels. Looking at trends for anaemia in adolescent girls (15-19 years), again 16 states/UTs show an incline. A sharp rise can be observed in Jammu and Kashmir (26.3 percentage points), Assam (24.3 percentage points), Tripura and Ladakh with 15.7 and 15.3 percentage points respectively.
Figure 5: Anaemia prevalence in women of reproductive age (15-49 years) in the 22 states/UTs
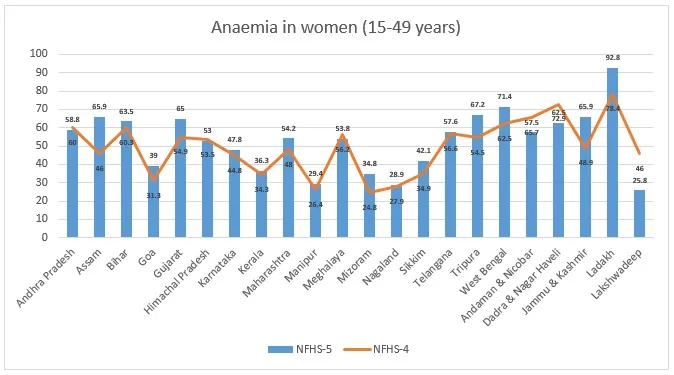 The highest prevalence of anaemia is observed in Ladakh, with 92.5, 92.8 and 96.9 percent in children under-five, women in reproductive age (15-49 years) and adolescent girls (15-19 years) respectively. Anaemia during adolescent mothers has a lasting impact, posing the risk of maternal mortality, low birth weight and higher risk of anaemia in the newborn.
Figure 6: Anaemia prevalence in adolescent girls (15-19 years) in the 22 states/UTs
The highest prevalence of anaemia is observed in Ladakh, with 92.5, 92.8 and 96.9 percent in children under-five, women in reproductive age (15-49 years) and adolescent girls (15-19 years) respectively. Anaemia during adolescent mothers has a lasting impact, posing the risk of maternal mortality, low birth weight and higher risk of anaemia in the newborn.
Figure 6: Anaemia prevalence in adolescent girls (15-19 years) in the 22 states/UTs
 Assam seems to be performing poorly on all nutrition specific interventions, which is a cause for concern. As per the 2016-18 Comprehensive National Nutrition Survey, about 40 percent adolescent girls suffered from anaemia. A quarter of adolescent girls are deprived of the four school-based services including mid-day meal, bi-annual health checkup and deworming, and weekly iron and folic acid supplementation. NFHS-5 data indicates a wide variation on consumption of iron and folic acid supplementation by pregnant women, with Kerala at 67 percent and Nagaland at 4.1 percent. Various factors including level of education of mother and birth order influence the consumption of IFA among pregnant women.
Talking of indicators on infant and young child-feeding practices, exclusive breastfeeding has improved across states; however, early initiation of breastfeeding and complementary feeding has declined in many states. Not all is bad. The nutrition sensitive indicators on water and sanitation show marked improvement with increased coverage across states/UTs. Ante-natal care coverage has also has improved across 11 state/UT’s, with marked improvement in Bihar and Manipur, with Goa having the highest coverage at 93 percent. Antenatal care can help in reducing adverse health outcomes during pregnancy and childbirth. An analysis from NFHS-4, indicates lower maternal education, poor wealth quintile, and teenage pregnancies as some of the reasons for lower utilisation of ante-natal care services in India.
Successful stories of change across India suggest investment in girls and women and heightened delivery of health and nutrition interventions in bringing down malnutrition. A review on the approach to break the intergenerational cycle of malnutrition, suggests investing in nutrition over a life as it has an impact over generations. The National Nutrition Strategy calls for a life cycle approach, with focus on nutrition interventions during critical periods for improved growth and development.
India needs to act now for a healthy future generation!
Assam seems to be performing poorly on all nutrition specific interventions, which is a cause for concern. As per the 2016-18 Comprehensive National Nutrition Survey, about 40 percent adolescent girls suffered from anaemia. A quarter of adolescent girls are deprived of the four school-based services including mid-day meal, bi-annual health checkup and deworming, and weekly iron and folic acid supplementation. NFHS-5 data indicates a wide variation on consumption of iron and folic acid supplementation by pregnant women, with Kerala at 67 percent and Nagaland at 4.1 percent. Various factors including level of education of mother and birth order influence the consumption of IFA among pregnant women.
Talking of indicators on infant and young child-feeding practices, exclusive breastfeeding has improved across states; however, early initiation of breastfeeding and complementary feeding has declined in many states. Not all is bad. The nutrition sensitive indicators on water and sanitation show marked improvement with increased coverage across states/UTs. Ante-natal care coverage has also has improved across 11 state/UT’s, with marked improvement in Bihar and Manipur, with Goa having the highest coverage at 93 percent. Antenatal care can help in reducing adverse health outcomes during pregnancy and childbirth. An analysis from NFHS-4, indicates lower maternal education, poor wealth quintile, and teenage pregnancies as some of the reasons for lower utilisation of ante-natal care services in India.
Successful stories of change across India suggest investment in girls and women and heightened delivery of health and nutrition interventions in bringing down malnutrition. A review on the approach to break the intergenerational cycle of malnutrition, suggests investing in nutrition over a life as it has an impact over generations. The National Nutrition Strategy calls for a life cycle approach, with focus on nutrition interventions during critical periods for improved growth and development.
India needs to act now for a healthy future generation!
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Dr. Shoba Suri is a Senior Fellow with ORFs Health Initiative. Shoba is a nutritionist with experience in community and clinical research. She has worked on nutrition, ...
Read More +


