
-
CENTRES
Progammes & Centres
Location
Nagaland needs a sociopolitical vision on health governance.

When compared to other Northeastern states, Nagaland fares very badly in terms of primary healthcare services utilisation. The National Family Health Survey 2016 highlights the dismal state of maternal and child healthcare. It has the lowest proportion of pregnant women (25%) who have received antenatal care in the first trimester of pregnancy. In fact, on this indicator, even Bihar (35%) exceeds Nagaland by 10 percentage points.
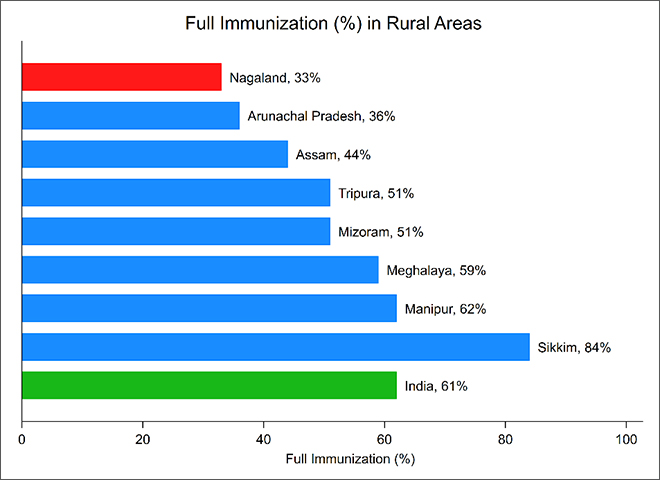
A ranking of the Northeastern states on key maternal and child health and healthcare indicators often places Nagaland at the bottom of the list. Nagaland is ranked the lowest among all of Northeast in case of institutional delivery and full immunisation coverage. Likewise 2006, Nagaland has continued to be the lowest in 2016 as well. Unlike other Northeastern states, Nagaland has registered no gains from India’s flagship National Rural Health Mission (NRHM) between 2006 and 2016 even after being a focus of the programme.
Nagaland is ranked the lowest among all of Northeast in case of institutional delivery and full immunisation coverage.
Ranking of Northeast states in institutional delivery and full immunisation, NFHS-III, 2006 and NFHS-IV, 2016
| Institutional Delivery | Full Immunisation | |||||||
| NFHS 2006 | NFHS 2016 | NFHS 2006 | NFHS 2016 | |||||
| % | Rank | % | Rank | % | Rank | % | Rank | |
| Sikkim | 47 | 2 | 95 | 1 | 70 | 1 | 83 | 1 |
| Manipur | 46 | 4 | 69 | 5 | 47 | 3 | 66 | 2 |
| Meghalaya | 29 | 6 | 51 | 7 | 33 | 5 | 61 | 3 |
| Tripura | 47 | 3 | 80 | 2 | 50 | 2 | 55 | 4 |
| Mizoram | 60 | 1 | 80 | 3 | 47 | 4 | 51 | 5 |
| Assam | 22 | 7 | 71 | 4 | 31 | 6 | 47 | 6 |
| Arunachal Pradesh | 29 | 5 | 52 | 6 | 28 | 7 | 38 | 7 |
| Nagaland | 12 | 8 | 33 | 8 | 21 | 8 | 35 | 8 |
NFHS 2016 also shows that Nagaland has the lowest level of child immunisation in the country. Given such poor indicators, the NITI Aayog’s Healthy States, Progressive India Report on the rank of states and union territories identifies Nagaland with worst overall performance as well as poorest incremental performance. The state showed a reversal in achievement with lower scores in year of assessment (2015-16) than the base year (2014-15).
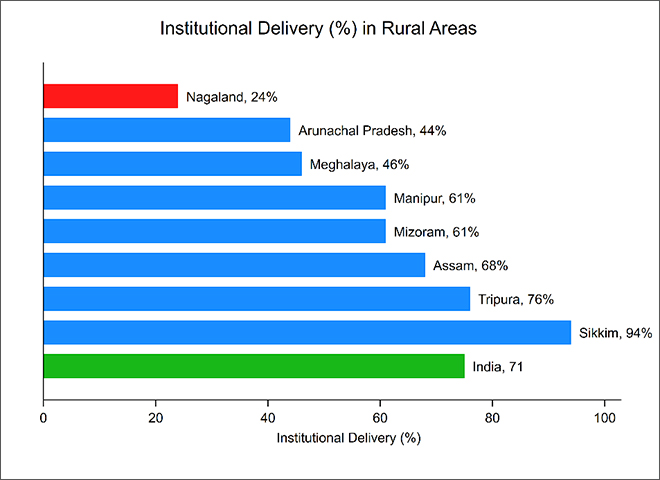
Healthcare utilisation in Nagaland is marked with substantial neglect particularly of the rural parts. In rural Nagaland, less than one-tenth of the pregnant women have reported of undertaking at least four ANC visits. A comparison of institutional delivery and full immunisation coverage across rural areas of the eight Northeastern states places Nagaland at the bottom of the list. The state of primary healthcare service utilisation is a huge concern across rural areas of Nagaland. Nagaland has recorded lowest coverage of institutional delivery and full immunisation in rural parts.
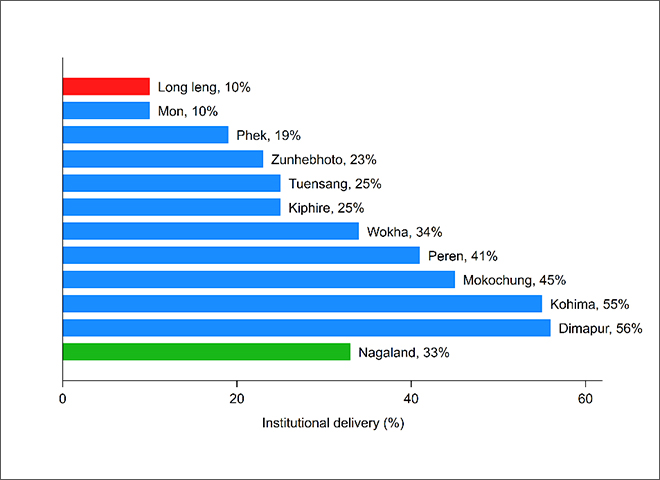
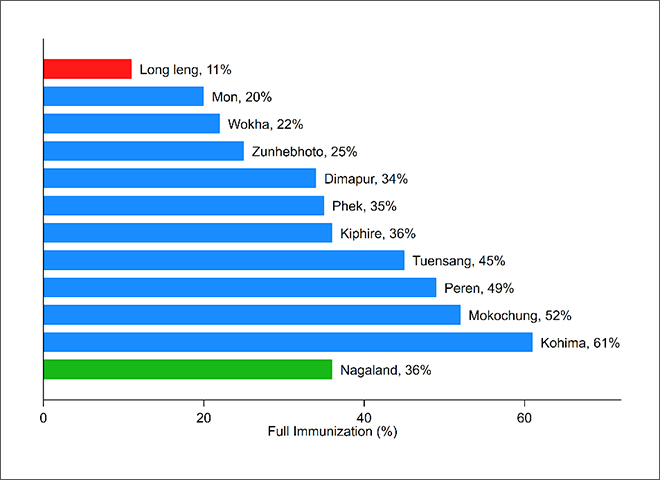
The hilly terrain of Nagaland is among the major concern in enabling rapid expansion of health infrastructure. This is reflected in terms of wide inter-district variations in these two elementary indicators of maternal and child health. The institutional delivery coverage in Kohima and Dimapur districts is more than five times that of Long Leng and Mon districts. Similarly, full immunisation coverage in Kohima is six times that of the most deprived Long Leng district. Such stark inter-district disparities are reflective of elementary developmental challenges including education, human resources, infrastructure as well as barriers both geographical as well as conflict-related.
The hilly terrain of Nagaland is among the major concern in enabling the rapid expansion of health infrastructure. This is reflected in terms of wide inter-district variations in these two elementary indicators of maternal and child health.
Figure: Districtwise perfomance on key indicators
A look at the outcome indicators show that the Nagaland health services haven’t been doing enough in a state that is enduring difficulties due to terrain, lack of private investments, internal conflict and misappropriation of development funds. A recent article in The Wire documents how massive central funding for health and development gets diverted and appropriated at various levels. The consequent state of health infrastructure further victimises the patient and their families who more often are helpless and have to undergo various hardships to seek quality healthcare. Research studies have also noted that the policies and initiatives such as JSY and JSSK are also less effective because of various impediments ranging from shortfall of medical staff to poor state of rural health infrastructure.
The Union Budget 2018 has catapult healthcare at the heart of the political discourse. This welcome shift in sociopolitical outlook was much awaited and should motivate states to do their bit in improving the daily lives of the citizens. The Union Budget has a substantial focus on improving service provisioning at health sub-centres by expanding the quantity and quality of services through establishment of newly proposed ‘health and wellness centres’. However, Nagaland needs a sociopolitical vision on health governance. In this respect, two areas are of utmost priority. First, the state should ensure availability of adequate health personnel in designated health centres in each of the districts. With improvements in human resources for health the state can conceive plans for uplifting the quality of medical care and diagnostic services at public health facilities. Second, women empowerment is critical to achieve the transition from a demand side perspective. Most of the well-performing states have high levels of female literacy whereas in Nagaland only one in every three women in the reproductive age group (15-49) has completed 10 or more years of schooling. Such poor educational profile is further associated with a high total fertility rate and huge unmet need for family planning services.
Time and again, the development community and the media has drawn attention towards the dismal state of health affairs in Nagaland. It is now for the government to reciprocate with policies and intent to improve health of the citizens.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Shalini Rudra was an Associate Fellow with Observer Research Foundation's (ORF) health initiative. Her primary research interest is in examining gender relations in health and ...
Read More +



