
-
CENTRES
Progammes & Centres
Location

Karnataka is one of the first Indian States to put a state health policy in place (2004). It has also been a pioneer in government supported health insurance schemes, with Yashaswini (2002) and Vajpayee Aarogyasri (2010) among the first initiatives in India. Among the larger States of India, Karnataka has one of the lowest Infant Mortality Rates (IMR) at 24 per 1000 live births, barring Kerala, Delhi, Maharashtra, Punjab and Tamil Nadu. The percentage of births in a health facility has increased dramatically in the 10 years from 65% in 2005 to 94% in 2015. Maternal Mortality Ratio (MMR), however, is still relatively worse and Karnataka’s MMR of 133 per 100000 live births is the highest among the South Indian States. Experts observe that the State has been able to close social and religious gaps in terms of income distribution, better than many other States.
Karnataka has a strong track-record in the formulation of health policies. It is often noted that the Karnataka Private Medical Establishments Act 2007 with the aim of registering private hospitals and monitoring their functioning was enacted even before the Clinical Establishment Act 2010, a central legislation which mainstreamed the discussion of private sector regulation. The revised Karnataka Private Medical Establishments (Amendment) (KPME) Act, 2017 was passed and received the governor’s nod in January 2018.
In addition, Karnataka revised its State Health Policy (2004) and renamed it the Karnataka Integrated Public Health Policy (2017). The stated aim of the new policy is “to establish a technically sound political, economic, social and legal framework that gives clear long-term directions and support to improve the health status of the people of Karnataka.” Reportedly, in 2017, Karnataka also became the first State in India to roll out Universal Health Coverage (UHC) by assuring health for its population of over 60 million under the Arogya Bhagya scheme by merging existing health schemes under a single umbrella.
However, ambitious-sounding policy conversations notwithstanding, the actual performance of the State in terms of health and nutrition outcomes leaves much to be desired.
The analysis of data has shown that despite the rhetoric, actual investments in health by the State have been quite low. Research by Brookings India showed that despite many ongoing health schemes, Karnataka’s per capita health spending by the State government was a low Rs 791, when compared to levels of spending in neighbouring States -- Rs 1022 in Andhra Pradesh, Rs 849 in Tamil Nadu or Rs 1070 in Kerala. Irrespective of many health insurance schemes, the National Sample Survey (2014) showed that only 10.5% of the State’s population was covered by any health insurance scheme. Out of pocket spending was 74.3% and 14.1% of households experiences catastrophic health expenditure, according to the Brookings India research.
Lack of sufficient spending in the health sector is evident from the analysis by the State government’s official publications as well. Graph 1, taken from the Karnataka Integrated Public Health Policy (2017), clearly shows that as a percentage of State domestic product as well as total expenditure, health spending has stagnated. More recent analysis has shown that as of 2017-18 (BE), Karnataka spent 3.8% of its aggregate expenditure on medical and public health and family welfare, which is lower than most other States in the country.
Graph 1: Health expenditure as a percentage of NSDP as well as total State expenditure
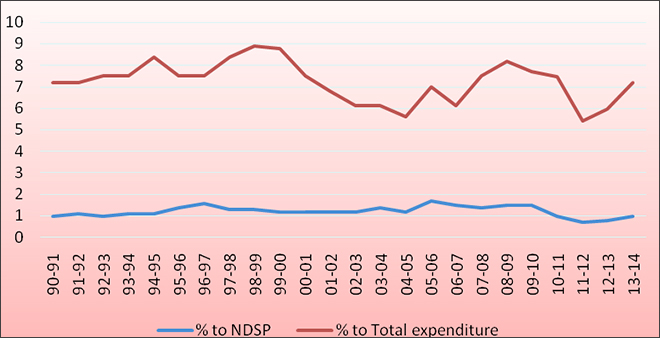 Source: Karnataka Integrated Public Health Policy (2017)
Source: Karnataka Integrated Public Health Policy (2017)
This paucity of funds, inevitably, seems to have had a negative impact on availability of medical infrastructure. According to Karnataka government’s own data in the latest Economic Survey of Karnataka (2017-18) given in Table 1, over the last seven years, hospital beds per lakh population has gone down considerably from 112 in 2010-11 to 80 in 2016-17. In fact, the current levels are even lower than what the State had achieved in 1970-71.
Table 1: Growth of health infrastructure in Karnataka
 Source: Economic Survey of Karnataka (2017-18)
Source: Economic Survey of Karnataka (2017-18)
Excluding Allopathy dispensaries.
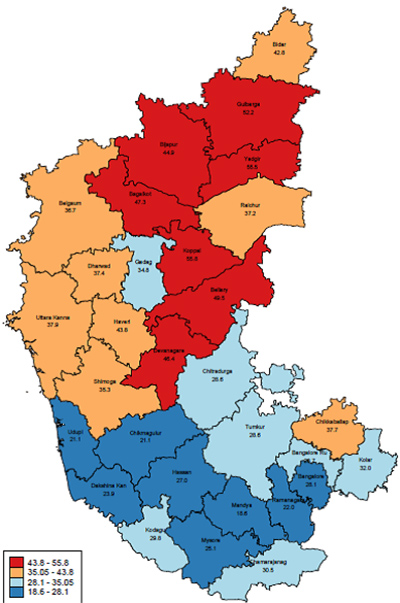
Map 1: Women aged 20-24 years married before the age of 18 years (%)
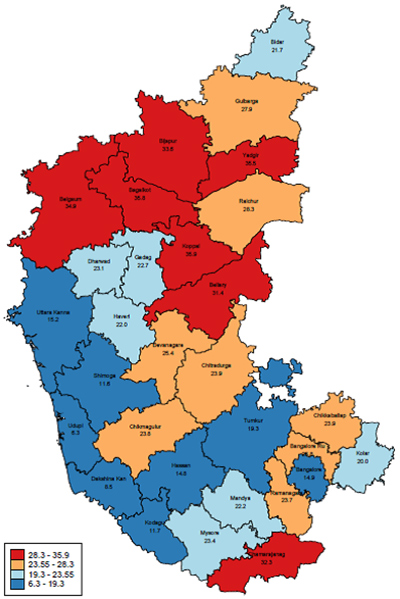 Source: NFHS-4 data
Source: NFHS-4 data
NFHS-4 findings show that nearly two-third (63%) households in the State live in a pucca house and almost all (98%) households have electricity. About one-third (34%) of households still practice open defecation. However, it is an improvement from the 53% open defecation barely a decade ago. Civil registration of births is almost complete in the State (95%). However, it is found that a high 21% women of age 20-24 years still got married before the legal minimum age of 18, although it is considerably down from 42% barely a decade ago. Nine percent of men aged 25-29 years got married before the legal minimum age of 21, down from 15 percent a decade ago. Map 1 shows the situation of under-age marriages in the districts – in many districts in the central northern part of the State and Chamarajanagar in the south, one in three girls are married before attaining legal age. It follows that of young women aged 15-19 in Karnataka, a very high 8 percent have already had a live birth or are pregnant with their first child. This indeed has severe impacts on the health of the mother as well as the child.
Unlike many other States, the IMR estimates from NFHS-4 are very close to the Sample Registration System estimates in Karnataka. IMR in Karnataka for the year 2014-15 is estimated at 28 deaths before the age of one year per 1,000 live births, down from 43 a decade ago. Infant mortality is 35 per 1,000 live births for mothers under legal age of marriage compared with 24 per 1,000 live births for mothers age 20-29. IMR is considerably higher in rural areas than urban areas, among Hindus than Muslims, and for scheduled tribes and scheduled castes than for others.
According to NFHS-4 findings, 70% of mothers in Karnataka had four or more antenatal care visits; Hindu women were much more likely to receive four or more antenatal visits than Muslim or Christian women. However, there are substantial inter-district differentials; percentage of mothers who had four or more antenatal care visits changed from 93% in Chikkaballapura district to a low 48% -- surprisingly -- in Bengaluru. However, it needs to be mentioned here that this level of inequity does not get reflected in case of institutional delivery- while the state average is 94%, the highest district has 99% coverage (Ramanagara) while the lowest district has a still impressive 80% coverage( Raichur).
Map 2: Children aged 12-23 months fully immunised (%)
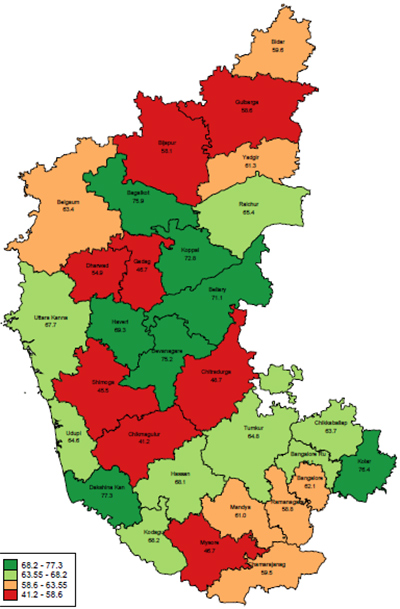 Source: NFHS-4 data
Source: NFHS-4 data
Immunisation coverage remains a major concern in the State as only less than two-thirds (63%) of children ages 12-23 months have received all basic vaccinations against six major childhood illnesses (tuberculosis, diphtheria, pertussis, tetanus, polio, and measles). This is all the more serious as Karnataka had achieved 60% full immunisation coverage in 1998-99 itself. A mere three percentage point improvement over almost two decades proves that policy efforts to tackle this major risk has been inadequate. Map 2 shows that there are worrying inter-district differentials in immunisation coverage. With a history of immunisation coverage actually dropping between 1998-99 (60%) and 2005-06 (55%), Karnataka will do good to have a comprehensive action plan to improve immunization numbers.
Map 3: Percentage of children wasted across Karnataka
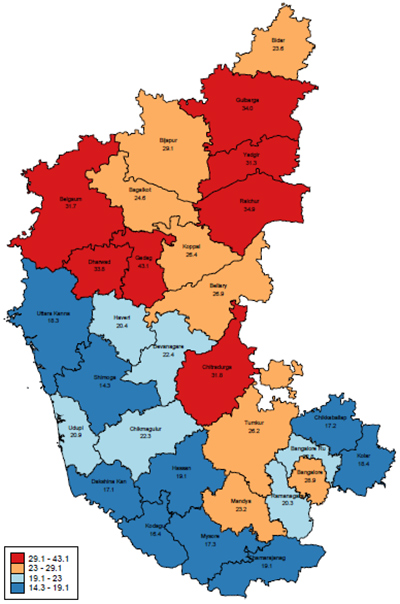 Source: NFHS 4 Data
Source: NFHS 4 Data
The nutritional status of Karnataka’s children leaves much to be desired. NFHS-4 results show that more than one-third (36%) children under five years of age are still stunted, or too short for their age. A similar percentage (35%) of children are underweight, prone to both chronic and acute undernutrition. While both stunting and underweight proportions have improved over the last decade, the main nutrition policy challenge of the State remains addressing the question of wasting, which is quite high, and worsening. 26% of Karnataka’s children are wasted, or too thin for their height. There has been an alarming increase in the percentage of children wasted in the State between 2005 (18%) to 2015 (26%). As Map 3 demonstrates, the proportions of children wasted shows considerable inter-district variations.
Map 4: Children stunted across Karnataka
 Source: NFHS 4 Data
Source: NFHS 4 Data
Map 4 shows that while stunting proportions have improved, in many districts of northern and central Karnataka, it is still a significant policy challenge. Many of these districts have very high stunting and wasting prevalence and will need focused attention through multi-pronged strategies. The Centre’s ambitious Ayushman Bharat and National Nutrition Mission are excellent opportunities for the State to enhance healthcare and nutrition service delivery. How the existing Arogya Bhagya scheme – Karnataka’s own UHC initiative -- will align itself with the National Health Protection Mission (NHPM) will be key. The forthcoming assembly elections provide an opportunity to mainstream health and nutrition policy debate in the State, going beyond rhetoric.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

Oommen C. Kurian is Senior Fellow and Head of the Health Initiative at the Inclusive Growth and SDGs Programme, Observer Research Foundation. Trained in economics and ...
Read More +
Rakesh Kumar is a Associate Fellow at ORF. He has done PGDCA (Post Graduation Diploma in Computer Application) from CMC, Delhi Centre and CIC(certificate in ...
Read More +


