The Covid-19 vaccination rollout has been slow in many parts of the world, and it might not be inaccurate to say that the newer, more transmissible variants have done a better job at immunising populations than the vaccine. More than 16 months since the global vaccination drive was started, wealthier countries have inoculated vastly higher proportions of their populations compared to the poorer ones. For example, as of late April 2022, the United Arab Emirates has administered 266 doses per 100 people; and Haiti, with a comparable total population, is at 2.3 doses per 100 people. Even when numerical disparities are high, however, a comparative country analysis might conflate equity with parity without considering the differences in demographic profiles—for which is often used the concept of “priority groups”, in terms of risk to the elderly and health workers on the frontlines. This report problematises this narrow definition of “priority groups”, and assesses vaccination data made available through global trackers. The aim is to examine the global experience of the Covid-19 vaccination effort, and measure the length and breadth of the remaining task for the international community.
Attribution:
Oommen C Kurian and Shoba Suri, “Covid-19 Global Vaccination Drive: The Goal of Equity in an Unequal World,” ORF Special Report No. 187, May 2022, Observer Research Foundation.
Introduction
Observers say that achieving vaccine equity during the Covid-19 pandemic has been a “stress test” for global health.[1]Since the outbreak of the pandemic in early 2020, policy conversations have seen “vaccine equity” emerge as a global catchword. In real terms, however, access to life-saving Covid-19 vaccines is strongly determined by both the overall economic status of the country, and the capacity of domestic pharmaceutical production. Billionaire and philanthropist Bill Gates, at the Munich Security Conference in February 2022 remarked that the Omicron variant of the novel coronavirus managed to do a better job of immunising populations in various regions of the world compared to vaccines, highlighting the inadequacy of the global vaccination drive.[2]In this sense, many experts believe that the world was “lucky” that Omicron caused less severe illness;[3]many countries, however, were still ill-prepared for the surge.
During the earlier, far more devastating Delta wave in the second quarter of 2021—as the wealthier countries mopped up limited supplies of Covid-19 vaccine doses—the World Health Organization (WHO) had warned that the world was on the brink of a “catastrophic moral failure”.[4]This is not to say that there has been no global effort to ensure vaccine coverage across countries during the pandemic. The WHO-led COVAX facility has, as of 28 April 2022, delivered more than 1.4 billion Covid-19 vaccine doses across 145 countries. More than eight of every 10 (85 percent) of these doses were shipped to the 86 lower-income countries participating in the COVAX Advance Market Commitment (AMC).[5]While laudable, these efforts have failed to bridge the wealth gap in vaccine access. The initial goal was to deliver 2 billion doses of vaccines worldwide in 2021 alone.
Covid-19 vaccines are life-saving technologies and global leadership and coordination is needed to overcome inequality. The “insurance scheme” approach of the COVAX initiative was a limited attempt where relatively wealthy countries pooled their resources to move towards an equitable distribution of vaccines; the effort has often been marred with roadblocks, including lack of transparency and inability to supply vaccines as committed.[6]The African Union, for example, is of the view that COVAX has failed in providing enough vaccines to large populations because the richer countries are getting hold of the biggest shares.[7]
The inability of COVAX to serve the requirements of all countries in need, can be blamed on its governance structure that tends to undermine the initiative’s equity goals.[8]Wealthier countries may have an immediate interest, fuelled by domestic political debates, to provide as many vaccines as possible to their citizens before even considering to share with other geographies—this is referred to as “vaccine nationalism”; they could also be using surplus vaccines to gain an advantage in other fields, in what is known as “vaccine diplomacy”.[9]Moreover, COVAX also has in its fold, pharmaceutical companies which are, ultimately, profit-motivated and who in some cases benefit from price differentiation.
A simple cross-country analysis of vaccine delivery that translates equity to parity would, however, be unrealistic considering the differences in countries’ demographic profiles. High-income countries indeed have bigger populations of the elderly, often living in nursing homes and whose non-communicable disease burden is also considerably larger as a proportion.[10]At the same time, majority of the population in these countries can afford to follow, and thereby gain from strict non-pharmaceutical interventions like lockdowns and self-quarantine. While in a crude sense, the prosperity of a society amplifies risks for Covid-19, they have also had disproportionally high access to pharmaceutical solutions, from medicines to vaccines, compared to poorer countries.
For India, its reported Covid-19 death rates have been worse than those of its South Asian neighbours. This is possibly because despite the average population being young and old people living with dispersed families, in terms of risk factors, India has the equivalent of many islands of Europe spread across a large sea of South Asia. Although the benefits of non-pharmaceutical interventions accrued largely to the well-off population and costs were mostly borne by the poorer sections, India has tried to make its vaccination drive more inclusive. This has resulted in high levels of coverage, indeed, nearly universal. This special report makes an assessment of comparable data made available by credible global trackers of vaccine equity, such aspandem-ic.com, curated by Philip Schellekens, a Senior Economic Adviser at the World Bank Group, andourworldindata.org, a project of the Global Change Data Lab, a registered charity run by a group of academics in the United Kingdom.
The Broad Context of Vaccine Inequity
WHO’s global Covid-19 vaccination strategy is aimed at minimising deaths and severe disease, and the overall disease burden; curtailing the impact on health systems; allowing for the full resumption of socio-economic activity; and reducing the risk of new variants.[11]The strategy called for fully vaccinating at least 70 percent of the world’s population, including most adults, adolescents and those at risk of non-communicable diseases.
Most governments started with doses for those aged 60 and above, health workers, and people who are clinically vulnerable. After these ‘priority groups’ are vaccinated, there is a wider rollout among younger age groups. The Pfizer vaccine has been approved for everyone aged five and above in the EU, US, UK, and some other countries.[12]Children aged between five and 11 receive a smaller dose of the vaccine; and Sinovac is being used for children as young as three in China and Colombia.[13]
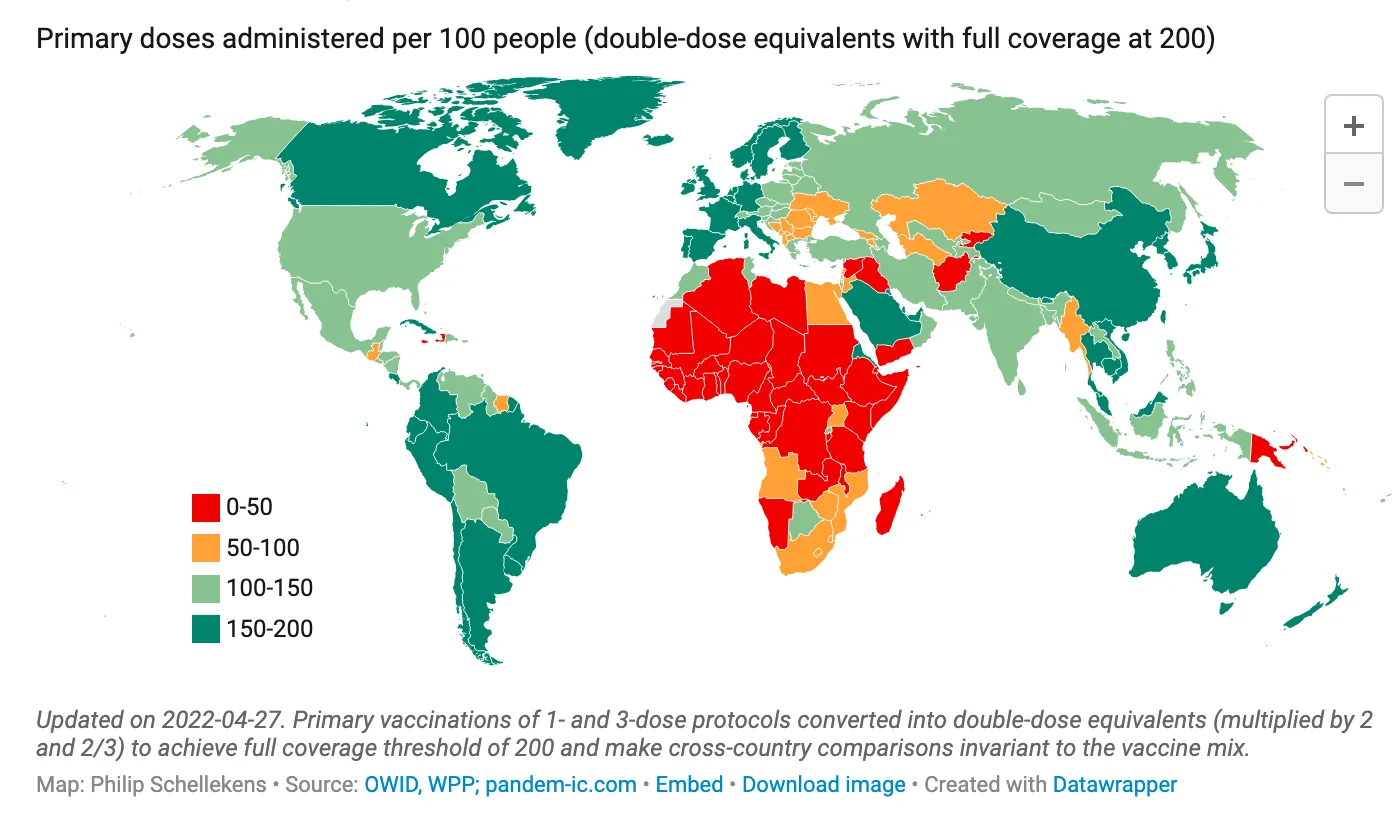
As of 28 April 2021, global trackers indicate that 184 countries have administered over 11.6 billion doses of a Covid-19 vaccine, more than two years after the first Covid-19 case was reported in China.[14]More than 5.12 billion people across the world—or 66.8 percent of global population—have received at least one dose of a Covid-19 vaccine. Map 1 shows the number of Covid-19 vaccine doses administered per 100 people. It illustrates how vaccine doses have yet to reach the poorer parts of the world.[15]
Map 1: Doses of Covid-19 Vaccines Administered per 100 Population
The gap between vaccination programs in different countries is stark: Africa has the slowest vaccination rate of any continent, with average doses per 100 population still under 50. About 63 percent of all shots worldwide have been administered in high- and upper-middle-income countries, as of 21 February 2022, and only one percent of these doses have been given in low-income countries. Of the combined population of low-income countries, a minuscule 11.4 percent have received at least one dose.[16]Some argue that even as the global vaccination distribution is skewed heavily towards HICs,[17]it is important to prioritise distribution to LMICs for equity and higher returns in maximising faster global coverage.
India—despite being a lower middle-income country with many poorer states larger in population than most countries—has managed to fully vaccinate more than 78 percent of its total population above 18 years of age. Although there are variations in coverage across states, high vaccine coverage along with a high seropositivity helped India maintain relatively low levels of mortality rates during the Omicron surge in January 2022.[18]The country has achieved higher vaccination coverage when compared to other countries with similar income levels mostly because of the domestic vaccine manufacturing capacity of Indian companies such as Serum Institute and Barat Biotech.
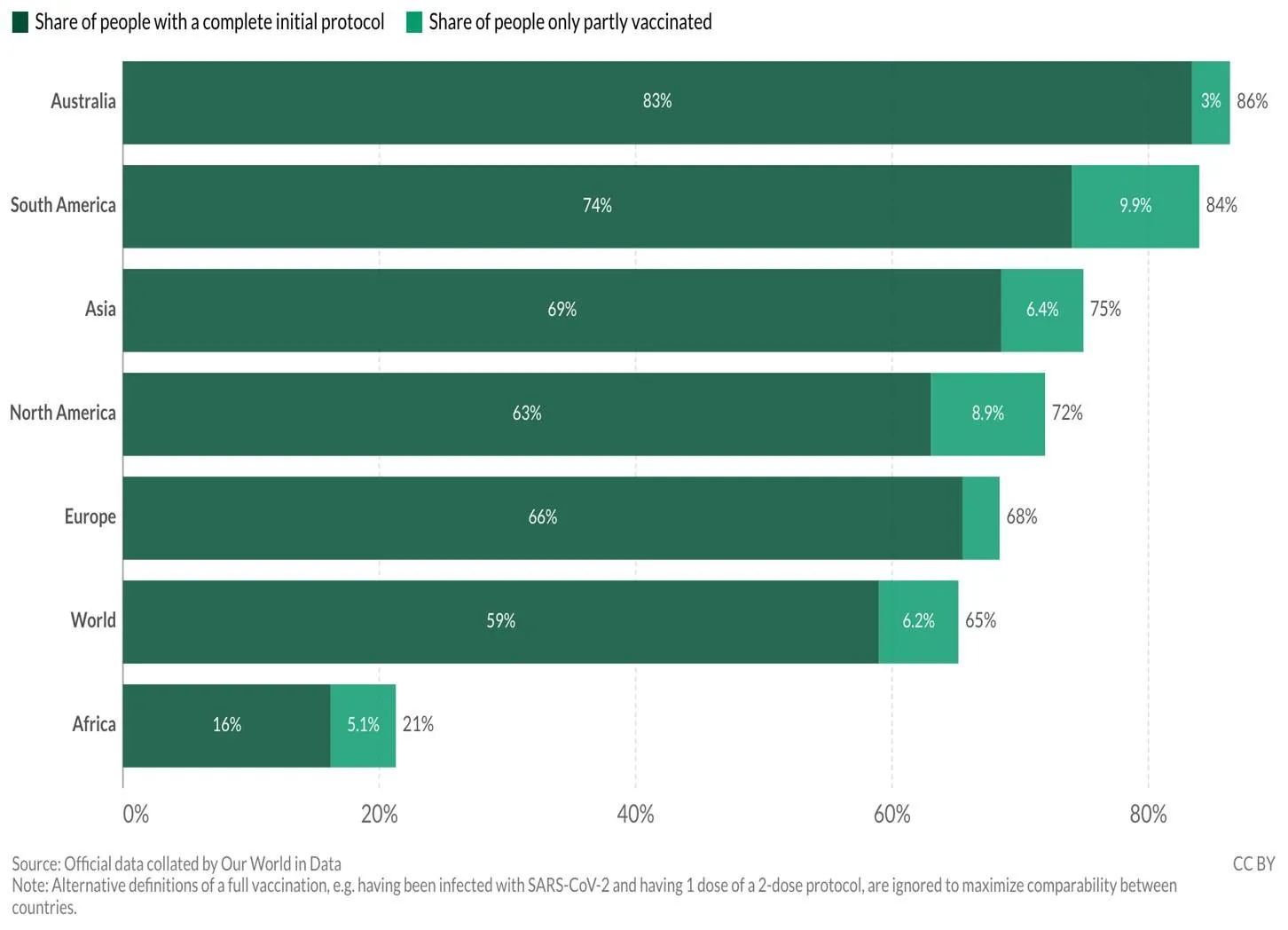
Broken down by region, Africa has the lowest number of people who have received at least one vaccine shot, at 21 percent (see Figure 1).
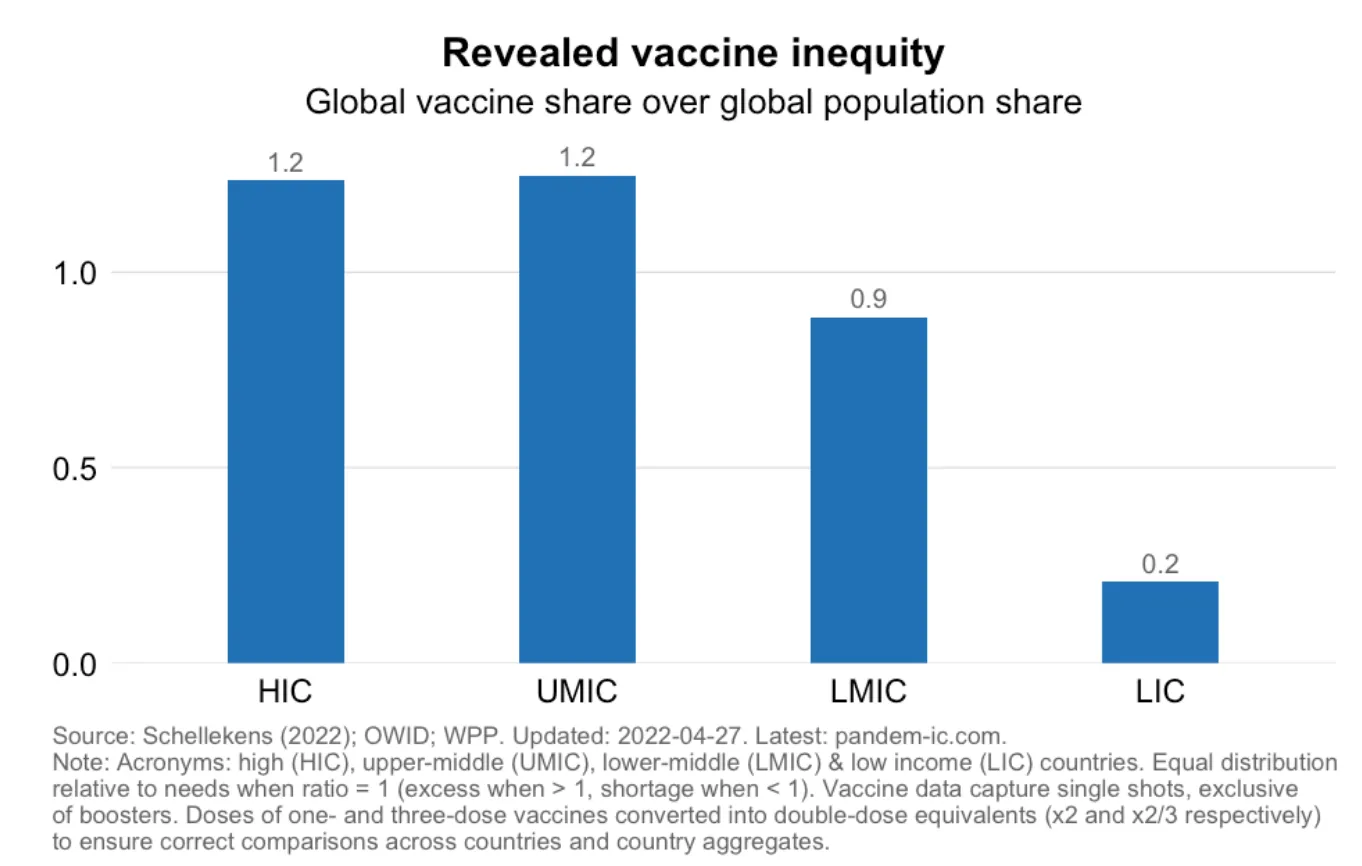
A useful tool for capturing current disparities in Covid-19 vaccination is the so-called Revealed Vaccine Inequity (RVI) ratio.[19]This metric is defined as the global vaccine share over the global population share, where any country or country group with a value above unity will have excess supply, and any with a value below unity will have a shortage of vaccines vis-a-vis global supply. Figure 2 shows the distance of various country groupings from an ideal equal global distribution. The higher-income and upper middle-income countries have a high global vaccine share at 1.2 compared to their respective populations; the LMICs have a share of 0.9; and the LICs have the lowest vaccine share at 0.2 percent compared to their populations. An economic intelligence report estimates that more than 85 poor countries will not achieve widespread vaccination coverage until 2023.[20]
The unequal distribution of Covid-19 vaccinations reflect massive social[21]and health-related inequalities across variables such as income, race, and ethnicity.[22],[23] Analysts also say that the disparities in vaccination rates across the World Bank country categories by income, reflect the effects of global accumulation of wealth. They are in line with existing disparities in average life expectancy. Indeed, inequality is often called the “handmaiden of progress”.[24] Evidence suggests that people of higher social positions are the first to take advantage of health-related progress, indicating a linear relationship between health inequalities and medical and technical developments.[25]
The imperative is to bridge the gaps. Studies indicate that equitable vaccine allocation strategies will help control the spread of new strains.[26] The UN has also highlighted the link between vaccine inequity and widening poverty gap. With extremely low doses administered to LICs (as seen in Figure 3), the repercussions will only contribute to growing inequalities between countries.[27]Lower vaccination trends in LMICs have in fact led to slower economic recovery. The UNDP says that lower-income countries will experience an increase in GDP if they were vaccinated at the same rate as higher-income countries.[28]
To be sure, the practice of “vaccine diplomacy” of certain countries has helped boost the supply of doses for populations in most need. For example, China’s global vaccine efforts have resulted in the availability of doses in many low- and lower -middle income countries.[29]Russia’s vaccine diplomacy, while less stable than China’s, has made its homegrown Sputnik available across Africa, West Asia, and countries like India as well with which it has partnered to enhance production capacity.[30]India’s own vaccine diplomacy has been ambitious in aiming to supply vaccines to poor countries.[31]Overall, however, these efforts were often limited to the respective realms of influence of the source countries.
Moreover, vaccination rates are determined not only by supply; acceptance and, conversely, hesitancy—plays a role. Indeed, widespread acceptance of Covid-19 vaccines is crucial for achieving sufficient immunisation coverage to end the global pandemic. Covid-19 vaccine acceptance across 15 survey samples covering 10 LMICs in Asia, Africa and South America, Russia (an upper-middle-income country) and the United States indicated higher willingness in LMICs as compared to United States and Russia.[32]In both the latter countries, the low vaccine acceptance is consistent with lower pre-pandemic childhood vaccination rates. The same survey found that although there was higher acceptance in LMICs, the respondents were concerned about the possible side-effects of the vaccine.[33]
It is important to understand why there would be hesitancy. After all, a lag in vaccination in any country could result in the emergence and spread of new variants that can then possibly overcome the immunity conferred by vaccines and prior disease.[34],[35]In HICs, vaccine hesitancy can be attributed to politicisation of the pandemic, overall, and fast-tracked vaccine development, in particular, which compounds skepticismper se.[36],[37]Messaging campaigns on vaccine efficacy and safety could be effective in further improving acceptance and addressing hesitancy in both HICs and LMICs. Making vaccines mandatory as a policy and spreading awareness on both, the benefits and side effects of vaccination can work to overcome vaccine hesitancy. There is evidence that information on the collective benefits of vaccination—i.e., herd immunity—is a stronger predictor of vaccine acceptance than emphasising on the benefit to an individual.[38]
The infrastructure can also play a role in how far the vaccination rollout can reach. In some countries, the inoculation drive has been hampered by difficulty in securing an appointment because of unstable internet connection, if at all.[39]
The ‘China and India Effect’
The presence of China and India in the UMICs and LMICs groupings, respectively, tends to skew the comparisons between vaccine coverage in the different country categories. An exercise where China and India are removed from their respective income-based country groupings will reveal their influence on the averages (see Figure 3).
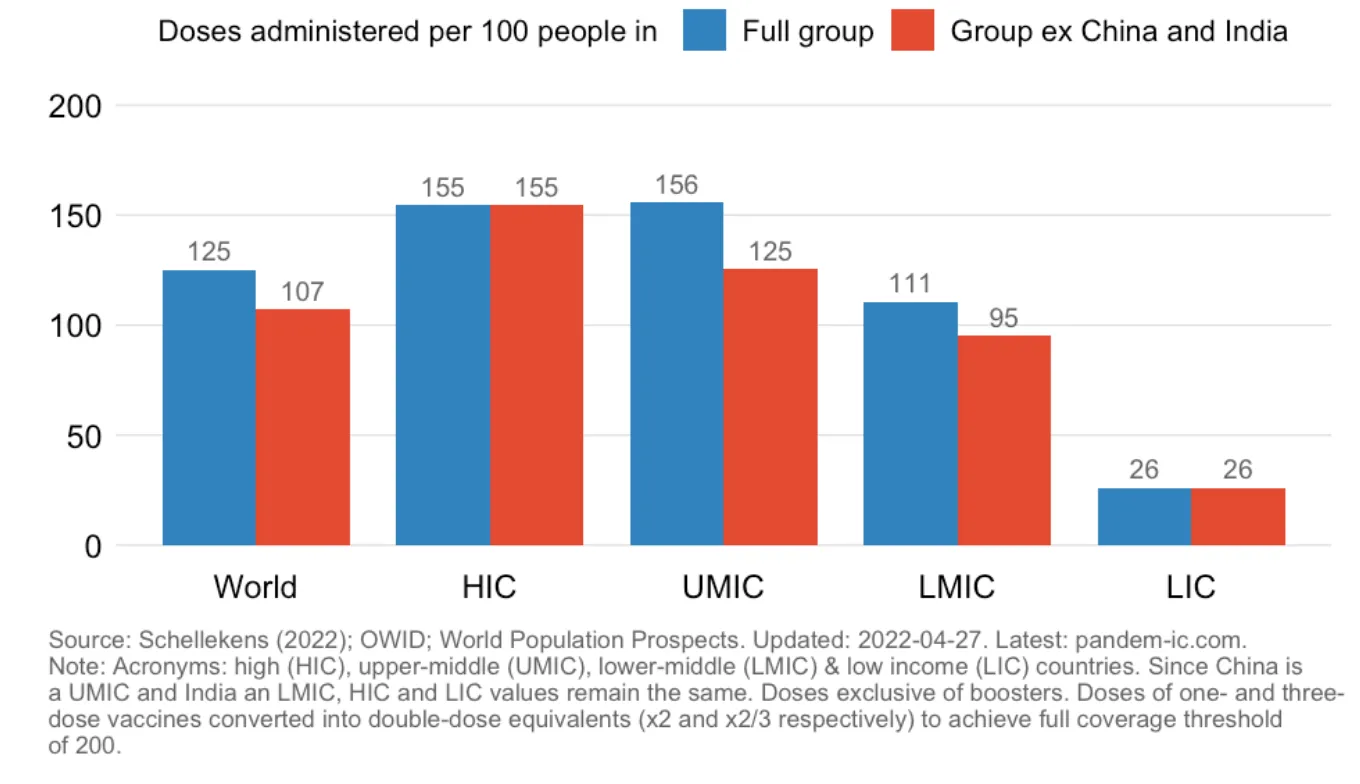
Figure 3: Vaccine Doses Administered Across Country Income Groups
As the figure shows, the averages for UMICs and LMICs are influenced by the respective achievements of China and India; when the two are removed from the analysis, global vaccine inequity becomes even more pronounced. The UMIC average falls from 156 to 125 doses per 100 people, and the LMIC average falls from 111 to 95—compared to the 155 doses per 100 people for HICs. That China and India are outliers in their respective country groupings is seen in the fact that almost 91 percent of the Chinese population, and 73 percent of the Indian population, have received at least one dose of Covid-19 vaccine—much higher than the respective country category averages, as seen in the figure.[40]
Parity Vs Equity
It can be argued that an unequal distribution of vaccines by itself need not signify vaccine inequity, since the risks of adverse outcomes of Covid-19 infections are determined by a variety of demographic, epidemiological, and socio-economic factors. For example, HICs who have received very high shares of vaccine doses also happen to be the country group with the highest proportions of the elderly population and those with specific non-communicable diseases that amplify Covid-19 risk. Thus, rather than aparitylens, a more nuancedequitylens based on needs may be better suited to assess the gaps in the distribution of vaccine doses.
Vaccine inequity amidst a virus-induced crisis is not new—in 2009, the swine flu pandemic demonstrated a similar situation of vaccine disparity. Covid-19 has only revealed the depths of global vaccine inequity.[41]Experts like Dr Sridhar Venkatapuram suggest that to prevent inequity of this scale from happening when the next pandemic arrives, the interests of the whole world—not just of the countries with the money and resources—need to be prioritised.”[42]Economic barriers to vaccine uptake are also amplified by mistrust, misinformation, and safety concerns.[43] There is a need to increase production capacity, supply chains, human resources, and health infrastructure to overcome the barriers in allocating and disseminating vaccines.[44]
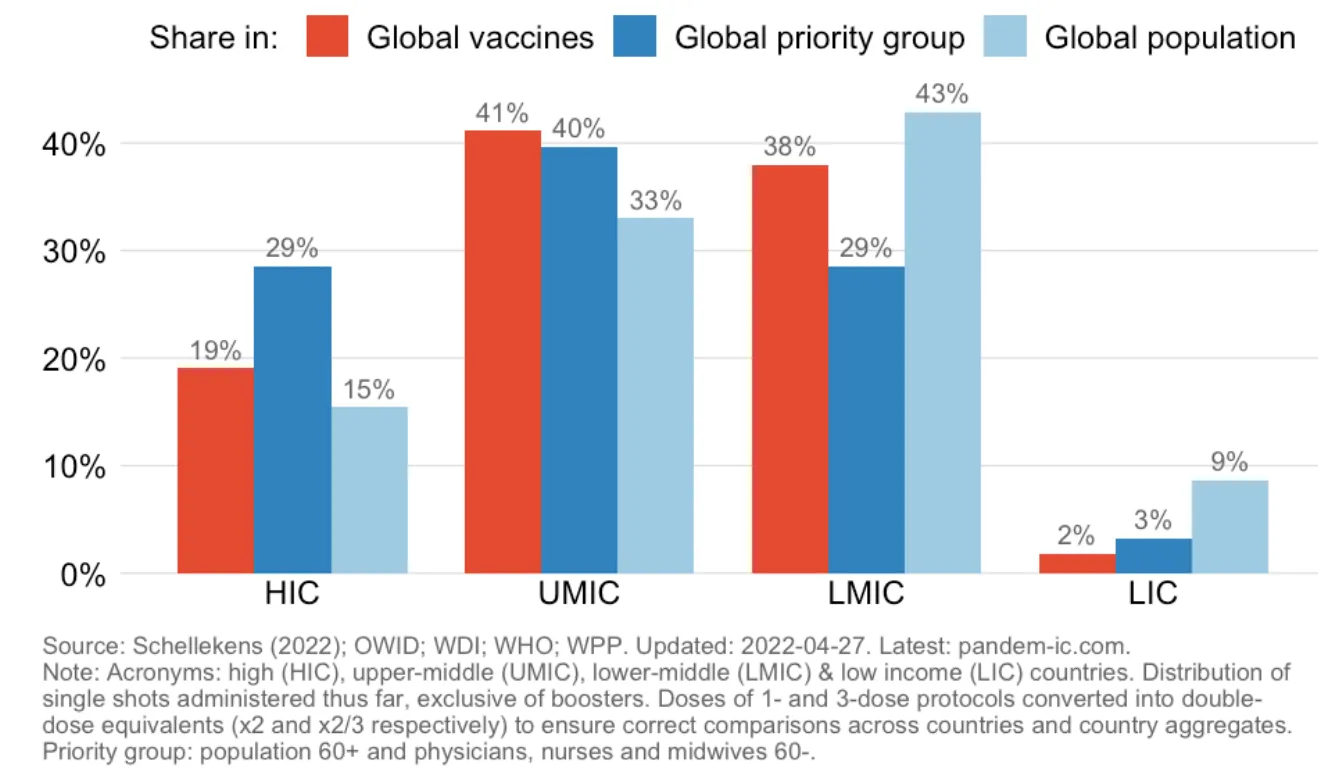
Figure 4 compares the global vaccine rollout against the distribution of global priority groups—defined primarily, owing to data limitations, as the vulnerable elderly population older than 60 years of age and medical professionals; as well as the global population distribution across income groupings. The higher-income countries account for 19 percent of doses administered globally; their priority groups comprise 29 percent of all global priority populations; and their combined population is 15 percent of global population. The higher middle-income countries (dominated by China) account for 41 percent of vaccine administered, 40 percent share in global priority groups and 33 percent of global population. On the other hand, lower-middle income countries (dominated by India) account for 38 percent of vaccine administered, 29 percent of priority groups and 43 percent share in global priority groups. As discussed briefly in an earlier section of this report, China and India have an enormous influence on the averages of their respective UMIC and LMIC groupings.
There is stark disparity in the numbers from the LICs. Just 2 percent of global vaccine supply has been received by low-income countries with 3 percent share of global priority groups and 9 percent of global population.
Here, it needs to be kept in mind that the proportion of both the elderly population, as well as health workers, are more likely higher in relatively better-off countries. For the sake of reasonable comparability, the global vaccination database (pandem-ic.com) excludes booster doses from its analysis due to the unavailability of data. This pushes down the relative proportion of the shares of vaccines of HICs and UMICs as these categories have already administered boosters to significant proportions of populations (a matter that will be discussed in a later section of this report).
Figure 4: Global Priority Groups Vs. Global Vaccine Distribution
The lower proportions of “priority groups” in the LICs can be attributed to lower life expectancy, weaker health systems, and, ironically enough, the migration of health workers from these same countries to the wealthier ones. This may lead to a counterintuitive theory: that vaccine inequity may not be as grave a problem as the global data on “priority groups” suggests.
Yet again, a more detailed examination, including of country-level data will change any such perception. Figure 5 assumes, because of unavailability of disaggregated data on vaccine doses administered, that all countries will prioritise the elderly and the health workers, and calculates vaccine doses administered per 100 persons from priority groups. Even assuming that all the doses were given to the priority groups, only 143 doses per 100 population of this category have been administered in LICs. Given that the data is normalised[45]to have a full coverage threshold of 200, this signifies that LICs have, as of 27 April 2022, received the volume of doses enough to fully vaccinate only around two-thirds of their elderly and health workers—a small share of their total population.
Jecker et al. (2021) in theJournal of Medical Ethicssuggests an ethical framework for distribution of Covid-19 vaccines based on priority groups—i.e., healthcare workers, and population above 65 years with co-morbidities at high risk of infection and death. Such global vaccine distribution strategy will help reduce health disparities and save lives.[46]The US health department, in its framework for equal distribution of vaccines, also emphasises focused administration to priority groups and ensuring vaccine equity in the domestic context.[47]
Figure 5: Sufficiency of Vaccine Doses to Cover Priority Groups
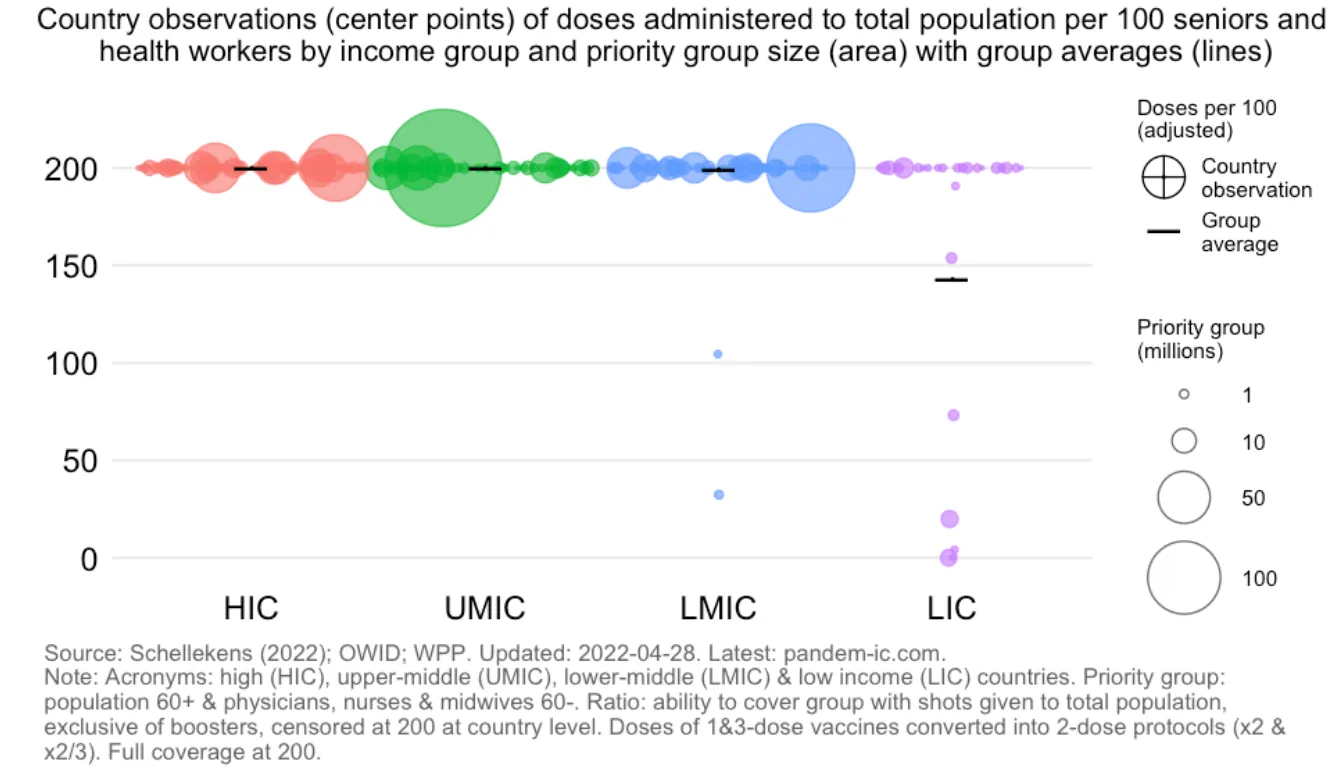
Similarly, when country-level numbers are disaggregated (Figure 6), it is clear that a handful of LMICs and many LICs have very low proportions amongst priority groups who have been covered by the vaccination rollout. Although the LIC average is 143 doses per 100 population, there are many countries in the grouping who have yet to cross 100. Notably, two of these countries at the bottom—with under 25 doses administered per 100 elderly and health workers—have considerably high numbers of these priority groups, as the bubbles indicate.
Figure 6: Sufficiency of Vaccine Doses to Cover Priority Groups: Country Data
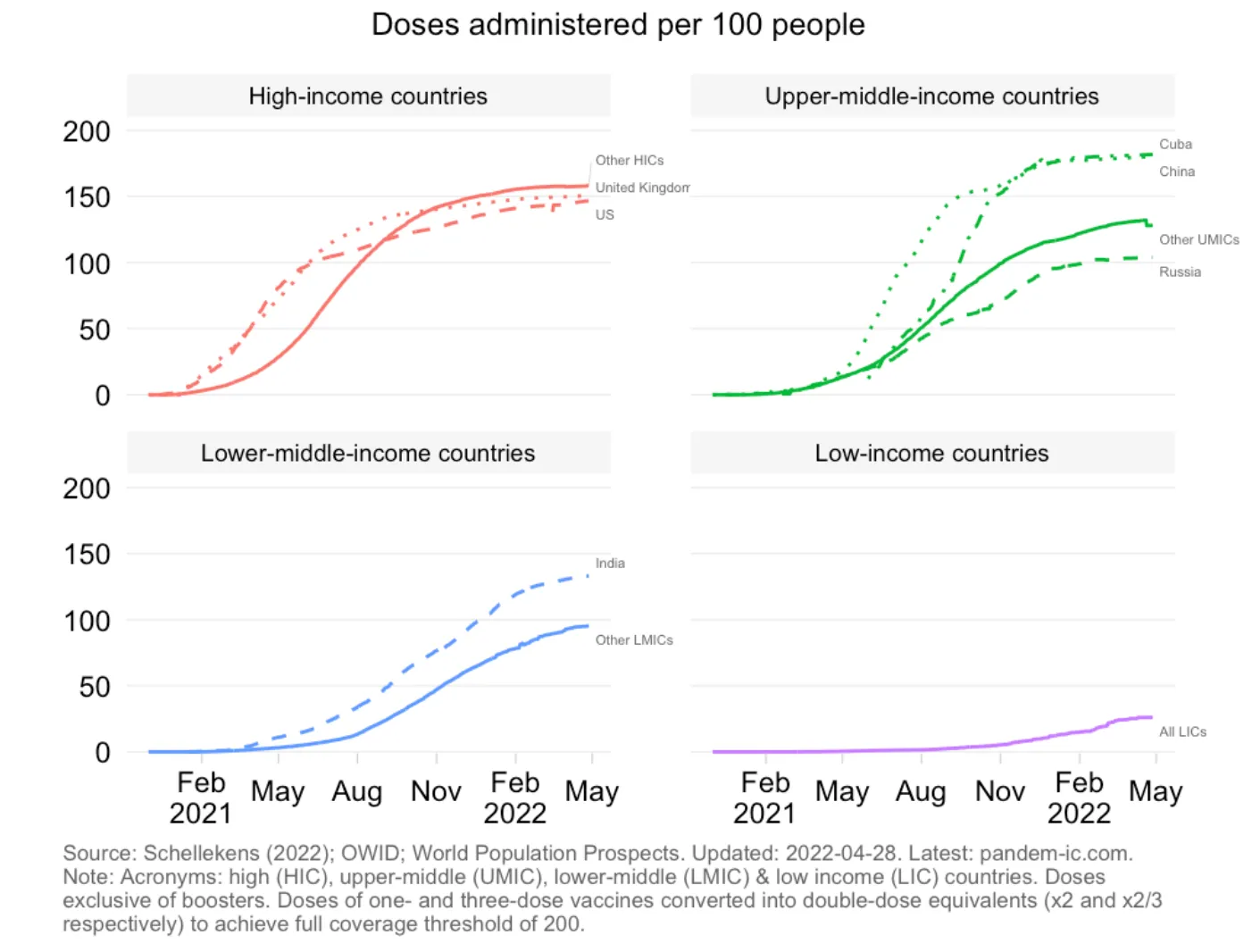
The level of global vaccine inequity in the past year is clearly visible when the doses administered per 100 population across the World Bank country classifications are tracked over time starting January 2021 (see Figure 7). The graphs show that it was only after the HIC vaccine rollout plateaued— due partly to vaccine hesitancy—that vaccine doses for poorer countries increased. The graphs also demonstrate what was mentioned briefly earlier about China and India being outliers in their UMIC and LMIC groups.
Figure 7: Global Vaccination Drive: Comparative Timelines
In an article in theLancetin July, Abecassis (2021) suggested that political leaders must address the “unacceptable” inequities in Covid-19 vaccine access between HICs and LMICs.[48]Covid-19 vaccination rollout in the better-off countries are now covering adolescents, whereas many LICs are still unable to vaccinate their healthcare workers and high-risk groups.[49]The Paris Peace Forum (PPF), an international platform dedicated to global governance has identified five priorities for universal Covid-19 vaccination: doses of Covid-19 vaccines must be shared globally; export restrictions on Covid-19 vaccines and components must be lifted; the need to scale-up manufacturing capacity for Covid-19 vaccines globally; regional and national surveillance and alert systems need to be improved; and adequate long-term pandemic financing is needed.[50]
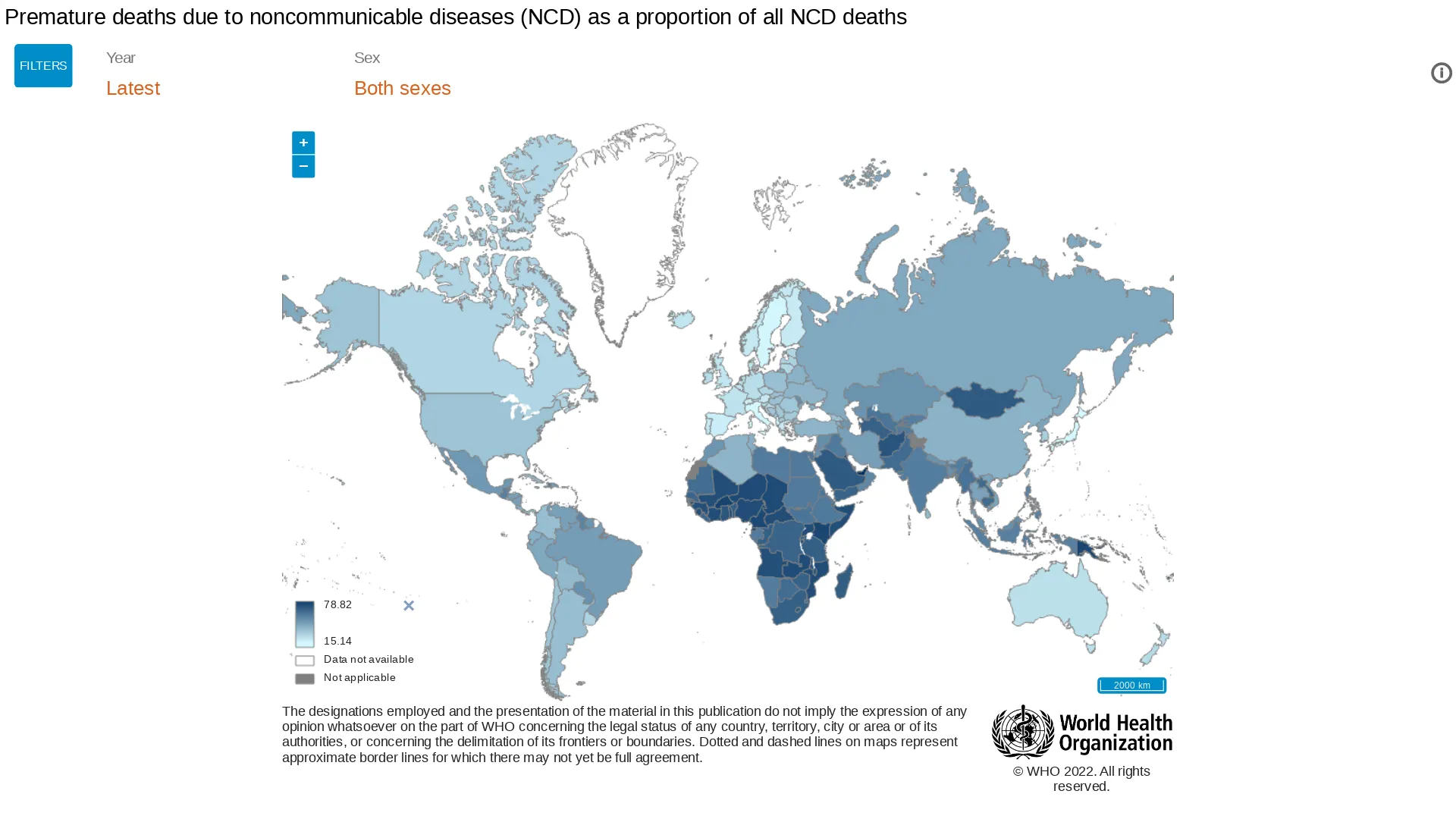
Importantly, there is a need to problematise the simplistic definition of “priority groups” across countries, which constitutes only those aged above 60 and all health workers (physicians, nurses and midwives) below 60.[51] Given the rapidly changing demographic and epidemiological profile of LICs and LMICs, it would be incorrect to assume that covering the elderly population already captures the amplified mortality risk that comorbidities present to the relatively younger populations in these countries. For example, Map 2 shows how a considerable proportion of NCD fatalities in many LICs and LMICs are relatively younger. In India’s case, 54 percent of all NCD deaths are categorised as “premature”, indicating that the risk is spread even across younger age groups. In Mumbai, a city for which age-wise Covid-19 mortality numbers are available, more than one-third of the total pandemic deaths were among non-elderly.[52]Clearly, the current definition of “priority groups” is inadequate. Nonetheless, lack of data necessitates that for now, global comparisons be made based on such minimalistic operational definitions that may tend to neglect certain nuances.
Map 2: Premature Deaths Due to Non-Communicable Diseases (NCD) as a Proportion of All NCD Deaths
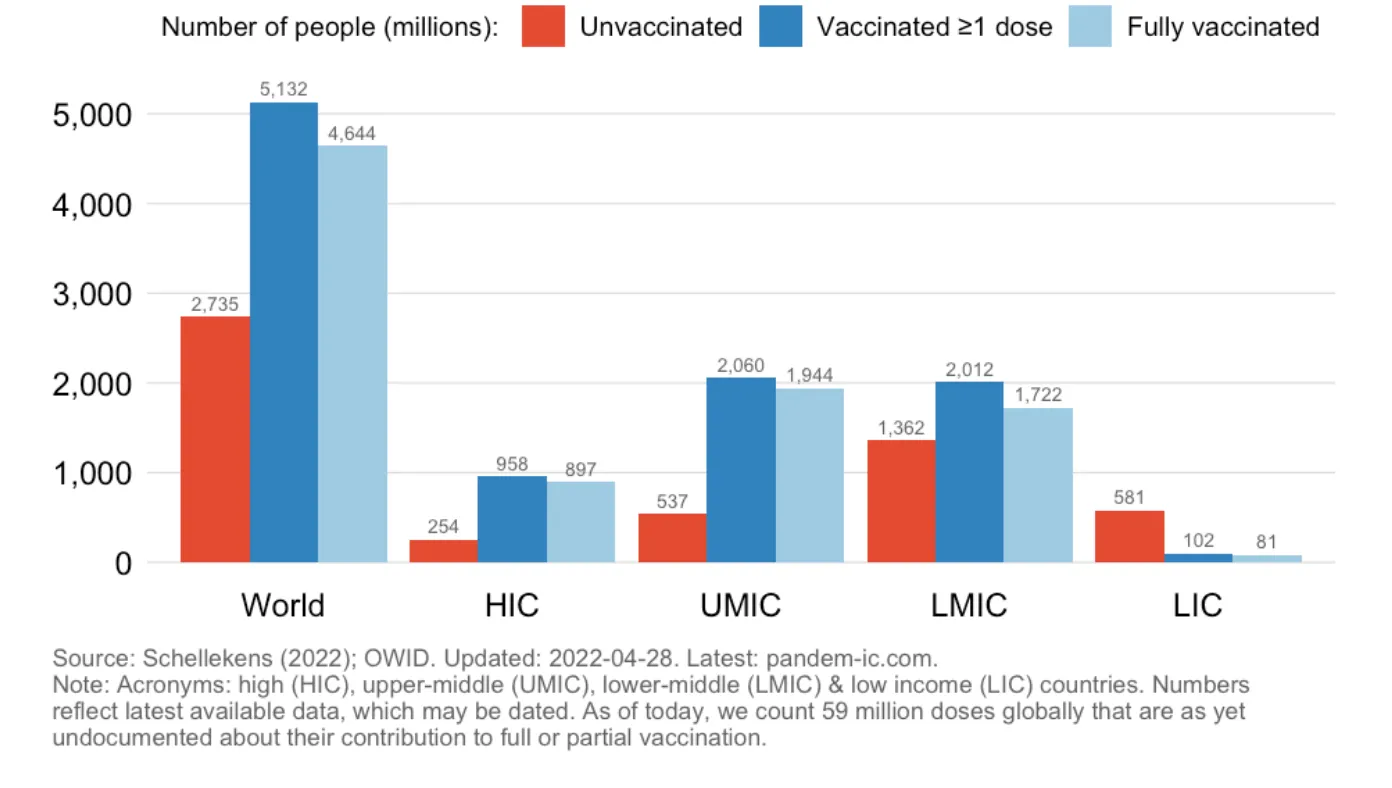
The current phase of the global vaccination drive, particularly in the relatively better-off countries, is dominated by the debate over boosters. As Figure 8 shows, as of 28 April 2022, a vast majority of the LIC population are still completely unvaccinated: just 81 million people are fully vaccinated, and a massive 581 million have not received even a single dose. In LMICs, while more than 1.7 billion are fully vaccinated, more than 1.3 billion remain completely unvaccinated. About half of the fully vaccinated 1.7 billion people from LMICs are from a single country: India. Indeed, in terms of the share of people vaccinated with at least one dose, India is close to the EU and US averages, as of 28 April 2022.[53] This also means that if India is removed from the picture, the LMIC situation will move closer to the LIC situation than what the graphs or averages show.
According to WHO, booster doses are administered to those who have completed a primary vaccination series—currently one or two doses (or three in some cases) of Covid-19 vaccine depending on the product—when, over time the immunity and clinical protection has fallen below a rate deemed sufficient in that population.[54]The objective of a booster dose is to restore vaccine effectiveness. According to the guidelines, improving coverage of the primary vaccination series should be prioritised over booster vaccination. The factors to be considered are waning immunity, vaccine effectiveness, global vaccine supply, and global and national equity.[55]
A study inLancetfinds that mRNA Covid-19 vaccines provide the biggest boost to antibody levels when given 10-12 weeks after the second dose. The study found that six of the seven boosters examined enhanced immunity after initial vaccination with Pfizer-BioNTech’s vaccine, while all seven increased immunity when given after two doses of AstraZeneca’s (AZN.L) vaccine. The authors call on countries to establish criteria for choosing booster vaccines based on immunological considerations, side-effects, availability, and the level of boost required for disease control.[56]
Meanwhile, an observational study from Israel on the effectiveness of a third dose of the mRNA Covid-19 vaccine for preventing severe outcomes, suggests that a third dose is effective in reducing severe Covid-19-related outcomes for patients who have received two vaccine doses at least five months earlier.[57]There is robust evidence for benefits of boosters; however, the marginal benefits for low-risk populations are low, compared to those of the primary vaccination series. Amidst supply constraints, WHO has referred to the broad-based booster programmes in wealthier countries to be “of concern”, from an equity point of view—especially the booster vaccination of sub-populations at lower risk of severe disease.[58]
Early studies suggest that the Omicron variant of SARS-CoV-2 is better able to evade vaccine protection than previous strains, though vaccination still offers strong protection against serious illness and hospitalisation.[59]A third booster dose of a vaccine does appear to offer protection against infection from Omicron and many countries have begun administering booster and fourth doses.[60]A study from England on booster vaccine with mRNA was found to be 85-95 percent effective against symptoms of Delta variant and 97-99 percent effective against hospitalisation and death.[61]
Figure 9: Booster Shots Administered Across the World
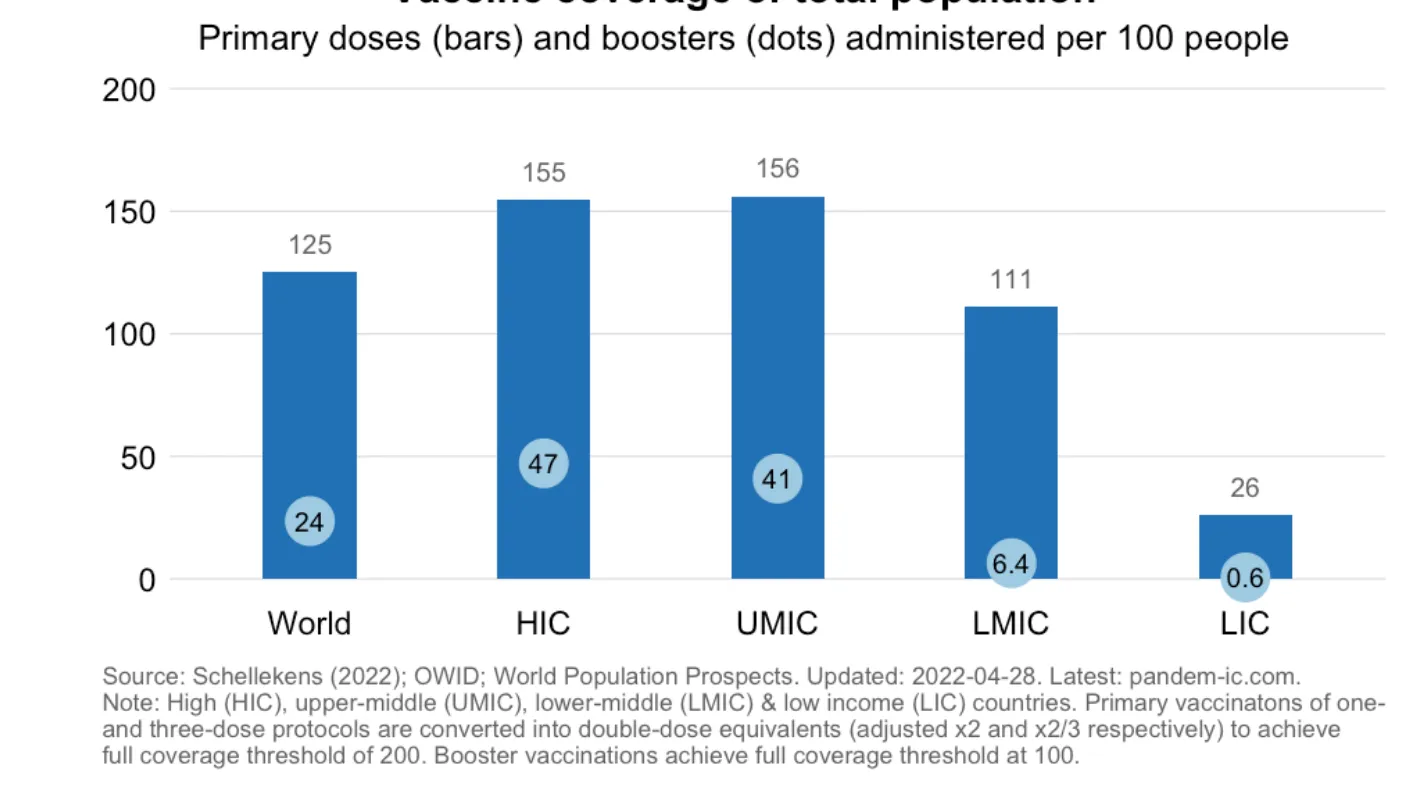
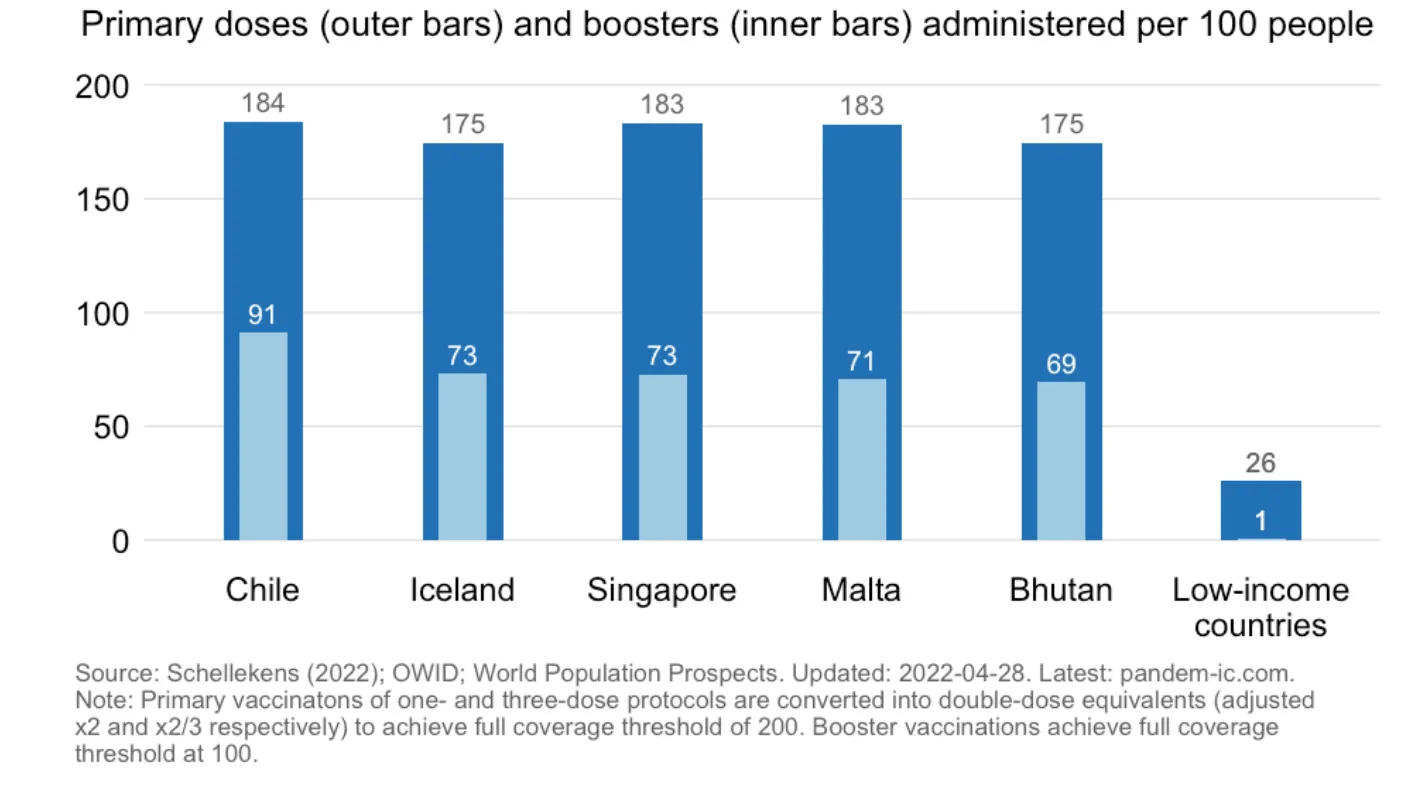
Figure 9 shows a comparative analysis of primary doses and booster doses administered per 100 population across the World Bank country groupings. Worldwide, 125 primary doses and 24 booster doses have been administered per 100 people. The booster doses are, predictably, the highest in HICs at 47 per 100 people, and lowest at 0.6in LICs. Taken as a proportion, almost double the number of primary doses per 100 population in LICs have been administered as boosters in HICs. Figure 10 shows the disaggregated country situation: many better-off countries are getting closer to the full population coverage threshold of booster doses of 100.
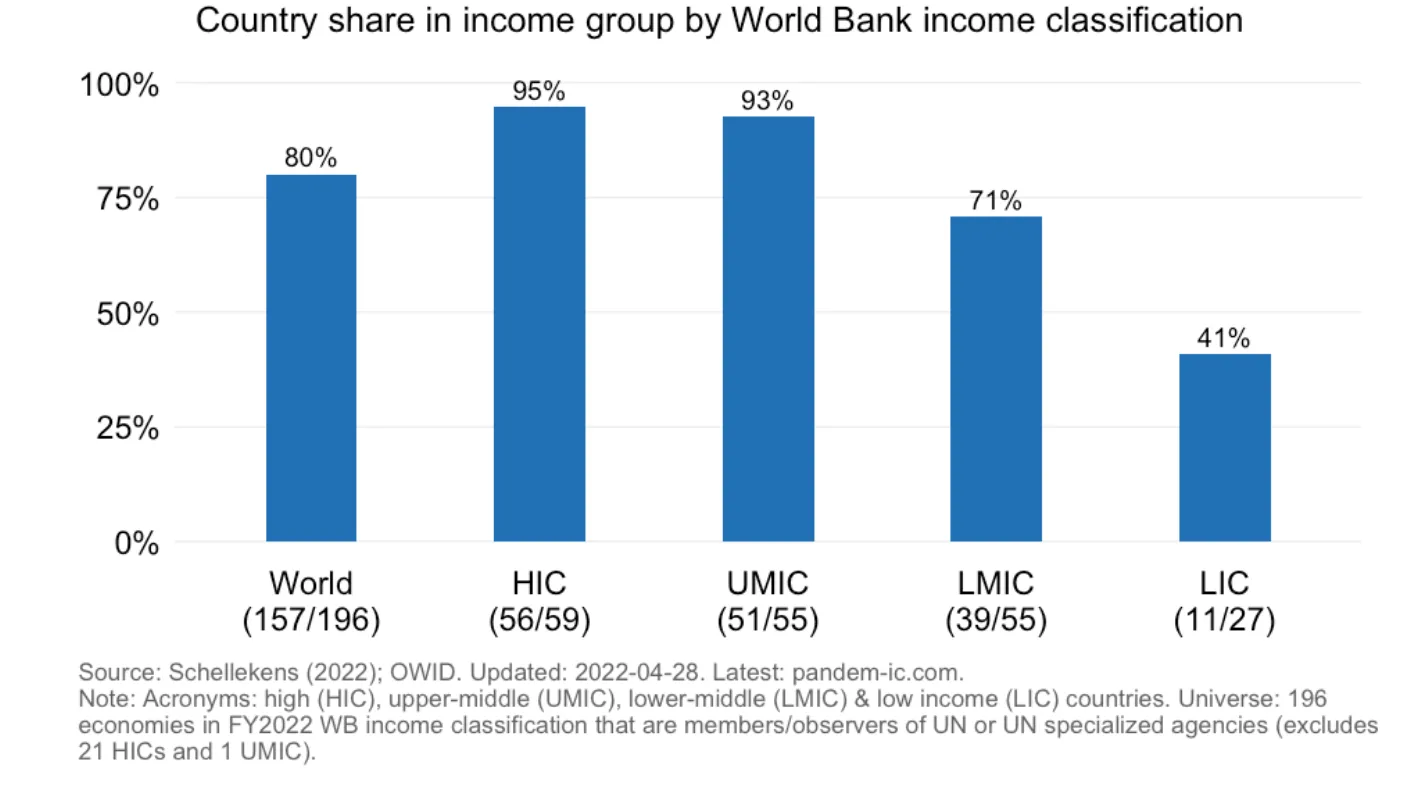
The number of countries managing to start booster coverage across income groupings is instructive as well. As Figure 11 demonstrates, most HICs (56 out of 59) have started administering boosters while only 11 out of 27 LICs have any coverage of booster doses among their populations. Starting from August 2021, HICs have rapidly ramped up boosting. UMICs and LMICs are closely following up on booster shots among respective populations. LICs have not even managed to find primary doses for their at-risk populations yet, even as a number have started administering booster doses. A descriptive study published in April 2022 on global diversity in Covid-19 vaccination points to widespread disparity and inequity specially in low-income countries. Using relevant data up till February, the study highlights the impact of this variance on immunity.[62]
Figure 11: Number of Countries with Booster Programs
As full vaccination and booster doses become the norm in the better-off countries, it would seem that the world has been divided into the vaccinated and the unvaccinated.[63]Where children with very low risk of severe infection, hospitalisation or death are eligible for booster doses in many countries, the need is for timely policy solutions that would give vaccine access to the vast millions of the “involuntarily unvaccinated”.
While efforts like COVAX and the Quad Vaccine Partnership[64]are commendable, most of the solutions to enhance vaccine access in the developing world still take the form of high-stakes bets on India’s vaccine manufacturing prowess.[65] Theinterim distribution forecastreleased in February 2021 by COVAX stated that 240 million of the 337.2 million doses to be distributed in the first half of the year were to be produced by India’s Serum Institute. Clearly, one of the main reasons why the global plans failed when India was overwhelmed by the Delta variant in the second quarter of 2021, was the over-dependence on a single manufacturing base. The intent was laudable; however, the humanitarian impulse of Western countries, made manifest through the COVAX facility, was mostly underwritten by India’s manufacturing capacity. It would prove costly for the global community.
As India met with a massive crisis brought about by the Delta variant and its vaccine exports got interrupted, UNICEF in June 2021 started a global campaign to urge developed countries with access to large numbers of doses to make donations to the rest of the world. Evidence suggests that generous donations of vaccines to LMICs can bring universal benefit.[66],[67]However, what reached the rest of the world often were leftover doses too close to their expiry date.[68],[69]As some experts in African countries have argued, this is perhaps time for the ethical management of Covid-19 vaccines, and addressing issues such as discrepancies in valuation of life, unethical pricing, and exploitation of vulnerable groups in clinical trials.[70]
The silver lining, as of writing this report, is that COVAX has gained pace and larger quantities are being exported to the LICs.[71] Moreover, Omicron being relatively “mild” ensured that the lack of vaccines in the poorer regions did not quickly escalate into an interminable tragedy to the extent the world feared. At the same time, vaccine “equity” resulting serendipitously from vaccine hesitancy of the rich would not be the solution the world needs. Scaling up manufacturing at geographically diverse bases is a non-negotiable. An important step would be the creation of an Access to Covid-19 Tools (ACT) accelerator-led global mRNA technology transfer hub. In mid-February 2022, it was announced that Egypt, Kenya, Nigeria, Senegal, South Africa and Tunisia will establish centres for mRNA vaccine production.[72]While this is welcome, the global experience of the past year would call for both vigilance and skepticism.
Oommen C. Kurian is Senior Fellow and Head of Health Initiative at ORF.
Shoba Suri is a Senior Fellow with ORF’s Health Initiative.
(The authors thank Amb Rakesh Sood, Dr Nilanjan Ghosh, Prof Shamika Ravi and Dr Samir Saran for their valuable inputs on an early draft of this paper, and Samanthi Sekar for her help with references.)
Endnotes
[1]Nicole De Paula and Cyan Brown, “Vaccine equity: a stress test for planetary health,”The Lancet Planetary Health5, no. 11 (November 2021): e758-e759.
[6]Jenny Lei Ravelo, “Is COVAX part of the problem or the solution?,”Devex,March 11, 2021, https://www.devex.com/news/is-covax-part-of-the-problem-or-the-solution-99334.
[7]Silence Charumbira, “Rich countries ‘ran off and secured supplies’ of Covid vaccines, says Africa envoy,”The Guardian,June 24, 2021, https://www.theguardian.com/global-development/2021/jun/24/rich-countries-deliberately-keeping-covid-vaccines-from-africa-says-envoy.
[8]Katerini Tagmatarchi Storeng, Antoine de Bengy Puyvallée and Felix Stein, “COVAX and the rise of the ‘super public private partnership’ for global health,”Global Public Health, An International Journal for Research, Policy and Practice,October 22, 2021, https://doi.org/10.1080/17441692.2021.1987502.
[9]“Coronavirus (COVID-19) vaccines for developing countries: An equal shot at recovery,”OECD,February 4, 2021, https://www.oecd.org/coronavirus/policy-responses/coronavirus-covid-19-vaccines-for-developing-countries-an-equal-shot-at-recovery-6b0771e6/.
[10] Clark, Andrew, Mark Jit, Charlotte Warren-Gash, Bruce Guthrie, Harry HX Wang, Stewart W. Mercer, Colin Sanderson et al. “Global, regional, and national estimates of the population at increased risk of severe COVID-19 due to underlying health conditions in 2020: a modelling study.” The Lancet Global Health 8,no. 8 (2020): e1003-e1017.
Wang, Wei, Qianhui Wu, Juan Yang, Kaige Dong, Xinghui Chen, Xufang Bai, Xinhua Chen et al. “Global, regional, and national estimates of target population sizes for covid-19 vaccination: descriptive study.” bmj 371 (2020).
[11]World Health Organization. “Strategy to achieve global Covid-19 vaccination by mid-2022.” (2021), https://cdn.who.int/media/docs/default-source/immunization/covid-19/strategy-to-achieve-global-covid-19-vaccination-by-mid-2022.pdf.
[12]“Pfizer and BioNTech Initiate Rolling Submission for Emergency Use Authorization of Their COVID-19 Vaccine in Children 6 Months Through 4 Years of Age Following Request From U.S. FDA,”Pfizer, February 1, 2022, https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-initiate-rolling-submission-emergency.
[13]AP, “China’s Sinovac says its vaccine is safe for children as young as 3,”Business Standard, March 23, 2021, https://www.business-standard.com/article/current-affairs/china-s-sinovac-says-its-vaccine-is-safe-for-children-as-young-as-3-121032301120_1.html.
[14]“More Than 11.3 Billion Shots Given: Covid-19 Tracker”,Bloomberg,April 5, 2022,
[15]Singh, Bawa, Vijay Kumar Chattu, Jaspal Kaur, Rajni Mol, Priya Gauttam, and Balinder Singh. “COVID-19 and Global Distributive Justice:‘Health Diplomacy’ of India and South Africa for the TRIPS waiver.” Journal of Asian and African Studies (2022): 00219096211069652.
[16]Mathieu, Edouard, Hannah Ritchie, Esteban Ortiz-Ospina, Max Roser, Joe Hasell, Cameron Appel, Charlie Giattino, and Lucas Rodés-Guirao. “A global database of COVID-19 vaccinations.”Nature human behaviour5, no. 7 (2021): 947-953.
[17]Wouters, O. J. et al. “Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation and deployment,”Lancet 397, 1023–1034 (2021).
[20]“More than 85 poor countries will not have widespread access to coronavirus vaccines before 2023,”Economist Intelligence, January 27, 2021, https://www.eiu.com/n/85-poor-countries-will-not-have-access-to-coronavirus-vaccines/.
[21]Bollyky, Thomas J., Christopher JL Murray, and Robert C. Reiner. “Epidemiology, not geopolitics, should guide COVID-19 vaccine donations.”The Lancet398, no. 10295 (2021): 97-99, https://doi.org/10.1016/S0140-6736(21)01323-4.
[23]Josh Holder, “Tracking Coronavirus Vaccinations Around the World,”The New York Times,April 4, 2022, https://www.nytimes.com/interactive/2021/world/covid-vaccinations-tracker.html.
[24]Rydland, Håvard Thorsen, Joseph Friedman, Silvia Stringhini, Bruce G. Link, and Terje Andreas Eikemo. “The radically unequal distribution of Covid-19 vaccinations: a predictable yet avoidable symptom of the fundamental causes of inequality.”Humanities and Social Sciences Communications9, no. 1 (2022): 1-6, https://www.nature.com/articles/s41599-022-01073-z.
[25]Glied S, Lleras-Muney A (2008) Technological innovation and inequality in health. Demography 45(3):741–761.
[26]Ye, Yang, Qingpeng Zhang, Xuan Wei, Zhidong Cao, Hsiang-Yu Yuan, and Daniel Dajun Zeng. “Equitable access to COVID-19 vaccines makes a life-saving difference to all countries.”Nature human behaviour6, no. 2 (2022): 207-216, https://www.nature.com/articles/s41562-022-01289-8.
[27]United Nations, “UN analysis shows link between lack of vaccine equity and widening poverty gap,” March 28, 2022, https://news.un.org/en/story/2022/03/1114762.
[28]UNDP Data Futures Platform, “ Impact of vaccine inequity on economic recovery,” February 2022, https://data.undp.org/vaccine-equity/impact-of-vaccine-inequity-on-economic-recovery-2022/.
[29]Darren Choi and Sean Janke, “ “Vaccine Diplomacy”? – China’s Global Vaccine Efforts and Controversies,” China Institute, University of Alberta, July 21, 2021, https://www.ualberta.ca/china-institute/news/the-latest/2021/july/vaccine-diplomacy.html.
[30]Samuel Ramani, “With Sputnik V, Russia Shot Itself in the Foot,”Foreign Policy,June 24, 2021, https://foreignpolicy.com/2021/06/24/russia-sputnik-v-vaccine-diplomacy-africa-prices-delays/.
[31]Bhattacharya, Sudip, Sheikh Mohd Saleem, Deep Shikha, Ozden Gokdemir, and Kedar Mehta. “Role of vaccine science diplomacy in low-middle-income countries for eradicating the vaccine-preventable diseases: Targeting the “LAST MILE”.”Journal of Family Medicine and Primary Care10, no. 8 (2021): 2739, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8483080/.
[32]Solís Arce, J.S., Warren, S.S., Meriggi, N.F.et al.“COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries,”Nature Medicine27, 1385–1394 (2021), https://doi.org/10.1038/s41591-021-01454-y.
[33]Solís Arce, Julio S., Shana S. Warren, Niccolò F. Meriggi, Alexandra Scacco, Nina McMurry, Maarten Voors, Georgiy Syunyaev et al. “COVID-19 vaccine acceptance and hesitancy in low-and middle-income countries.”Nature medicine27, no. 8 (2021): 1385-1394, https://www.nature.com/articles/s41591-021-01454-y.
[34]Sean Wei Xiang Ong, Barnaby Edward Young and David Chien Lye, “Lack of detail in population-level data impedes analysis of SARS-CoV-2 variants of concern and clinical outcomes,”THE LANCET Infectious Disease 21, no. 9, ( September 2021): 1195- 1197, https://doi.org/10.1016/S1473-3099(21)00201-2.
[35]“Public Health Measures to Suppress the Pandemic,”THE LANCET COVID-19 COMMISSION,February 2021, https://covid19commission.org/public-health-measures.
[36]Hornsey, M. J., Finlayson, M., Chatwood, G. & Begeny, C. T., “Donald Trump and vaccination: the effect of political identity, conspiracist ideation and presidential tweets on vaccine hesitancy,” J. Exp. Soc. Psychol. 88, 103947 (2020).
[37]Bokemper, S. E., Huber, G. A., Gerber, A. S., James, E. K. & Omer, S. B., “Timing of COVID-19 vaccine approval and endorsement by public figures,” Vaccine 39, 825–829 (2021).
[38]Sveinung Arnesen, Kristine Bærøe, Cornelius Cappelen and Benedicte Carlsen, “Could information about herd immunity help us achieve herd immunity? Evidence from a population representative survey experiment,”Scandinavian Journal of Public Health,May 9, 2018, https://doi.org/10.1177/1403494818770298.
[39]Marlene Cimons, “Getting a coronavirus vaccine appointment fills me with despair. Every search ends in frustration, and I’m at a low point of a long, dark year,”The Washington Post, February 5, 2021, https://www.washingtonpost.com/health/covid-vaccine-appointment-system-failure/2021/02/04/c7a5c300-6662-11eb-886d-5264d4ceb46d_story.html.
[40]Ritchie, Hannah, Edouard Mathieu, Lucas Rodés-Guirao, Cameron Appel, Charlie Giattino, Esteban Ortiz-Ospina, Joe Hasell, Bobbie Macdonald, Diana Beltekian, and Max Roser. “Coronavirus pandemic (COVID-19).”Our world in data(2020),https://ourworldindata.org/covid-vaccinations?country=OWID_WRL.
[41]Grace Browne, “2021 Revealed the Depths of Global Vaccine Inequity,”Wired, December 20, 2021, https://www.wired.com/story/2021-vaccine-inequity/.
[43]Weintraub RL, Subramanian L, Karlage A, Ahmad I, Rosenberg J., “COVID-19 vaccine to vaccination: why leaders must invest in delivery strategies now”, Health Aff (Millwood) 2021;40:33-41.
[44]Katz, Ingrid T., Rebecca Weintraub, Linda-Gail Bekker, and Allan M. Brandt. “From vaccine nationalism to vaccine equity—finding a path forward.”New England Journal of Medicine384, no. 14 (2021): 1281-1283, https://www.nejm.org/doi/full/10.1056/NEJMp2103614.
[46]NS Jecker, AG Wightman, DS Diekema, “Vaccine ethics: an ethical framework for global distribution of COVID-19 vaccines,”Journal of Medical Ethics47, no.5, (2021):308-317.
[49]African Union, Africa Centres for Disease Control and Prevention, “Latest updates from Africa CDC on progress made in COVID-19 vaccinations on the continent,” 2022, https://africacdc.org/covid-19-vaccination/
[53]Ritchie, Hannah, Edouard Mathieu, Lucas Rodés-Guirao, Cameron Appel, Charlie Giattino, Esteban Ortiz-Ospina, Joe Hasell, Bobbie Macdonald, Diana Beltekian, and Max Roser. “Coronavirus pandemic (COVID-19).”Our world in data(2020), https://ourworldindata.org/covid-vaccinations
[56]Munro, Alasdair PS, Leila Janani, Victoria Cornelius, Parvinder K. Aley, Gavin Babbage, David Baxter, Marcin Bula et al. “Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): a blinded, multicentre, randomised, controlled, phase 2 trial.”The Lancet398, no. 10318 (2021): 2258-2276,https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02717-3/fulltext.
[57]Barda, Noam, Noa Dagan, Cyrille Cohen, Miguel A. Hernán, Marc Lipsitch, Isaac S. Kohane, Ben Y. Reis, and Ran D. Balicer. “Effectiveness of a third dose of the BNT162b2 mRNA COVID-19 vaccine for preventing severe outcomes in Israel: an observational study.”The Lancet398, no. 10316 (2021): 2093-2100,https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)02249-2/fulltext.
[59]Cassandra Willyard, “What the Omicron wave is revealing about human immunity,”Nature Briefing,February 2, 2022, https://www.nature.com/articles/d41586-022-00214-3.
[60]“Factbox: Countries weigh need for COVID-19 booster shots,”Reuters, February 21, 2022,
[61]Andrews, Nick, Julia Stowe, Freja Kirsebom, Samuel Toffa, Ruchira Sachdeva, Charlotte Gower, Mary Ramsay, and Jamie Lopez Bernal. “Effectiveness of COVID-19 booster vaccines against covid-19 related symptoms, hospitalisation and death in England.”Nature medicine(2022): 1-1, https://www.nature.com/articles/s41591-022-01699-1
[62]Chen, Z., Zheng, W., Wu, Q.et al.,“Global diversity of policy, coverage, and demand of COVID-19 vaccines: a descriptive study”,BMC Med20, 130 (2022), https://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-022-02333-0
[63]Health-Europe, The Lancet Regional. “The Vaccinated and unvaccinated need to coexist with tolerance and respect.” The Lancet regional health. Europe 13 (2022): 100326.
[66]Ye, Yang, Qingpeng Zhang, Xuan Wei, Zhidong Cao, Hsiang-Yu Yuan, and Daniel Dajun Zeng. “Equitable access to COVID-19 vaccines makes a life-saving difference to all countries.”Nature human behaviour6, no. 2 (2022): 207-216, https://www.nature.com/articles/s41562-022-01289-8
[67]Yamin, Dan. “Vaccine inequality benefits no one.”Nature Human Behaviour6, no. 2 (2022): 177-178, https://www.nature.com/articles/s41562-022-01297-8
[70]Binagwaho, Agnes, Kedest Mathewos, and Sheila Davis. “Time for the ethical management of COVID-19 vaccines.” The Lancet Global Health 9, no. 8 (2021): e1169-e1171
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.
Dr. Shoba Suri is a Senior Fellow with ORFs Health Initiative.
Shoba is a nutritionist with experience in community and clinical research. She has worked on nutrition, ...

 PDF Download
PDF Download