
This article is part of the series Children and the Pandemic: An Analysis Across Countries
Immunisation is key to child survival and is a cost-effective way of protecting the lives of children. Each US $1 invested in child immunisation brings a return of US $44 for low- and middle-income countries. With the looming threat of the pandemic, 23 million children globally have missed out on routine immunisation in 2020. The pandemic has further worsened the worrying trends on immunisation against preventable child illness. A recent review on the impact of COVID-19 on immunisation campaigns and programmes suggests a reduction in both coverage and number of vaccines administered due to lockdown restrictions, shortage of health workers, and resource diversion to address the pandemic.
Immunisation coverage data shows a plateau over decades, with global coverage of 83 percent and increase in unvaccinated by 3.4 million in 2020. The recent modelling study by Lancet finds a tenacious gap in vaccine coverage by end of 2020, extending through to 2021. Findings estimate a dip in coverage for diphtheria-tetanus-pertussis (DTP) 3 at 76·7 percent and measles vaccine at 78·9 percent in 2020. India experienced a large drop in DTP3 vaccine coverage from 91 to 85 percent. According to recent data released by WHO-UNICEF, over 3 million children in India have missed out on ther first dose of DTP in 2020, more than double the number of children in 2019.
A recent review on the impact of COVID-19 on immunisation campaigns and programmes suggests a reduction in both coverage and number of vaccines administered due to lockdown restrictions, shortage of health workers, and resource diversion to address the pandemic.
India has seen tremendous progress in immunisation coverage through its Mission Indradhanush programme (now Intensified Mission Indradhanush-IMI), targeting 27 million new borns and 29 million pregnant women annually. Regardless of this, infectious diseases continue to contribute to a significant proportion of child mortality and morbidity in India. According to the Pneumonia and Diarrhoea Progress report 2020, nearly half a million pneumonia and diarrhoea deaths occur in India followed by Nigeria. India can markedly reduce pneumonia and diarrhoea deaths through an integrated package of interventions—exclusive breastfeeding, immunisation, improving water and sanitation, and reducing exposure to air pollution.
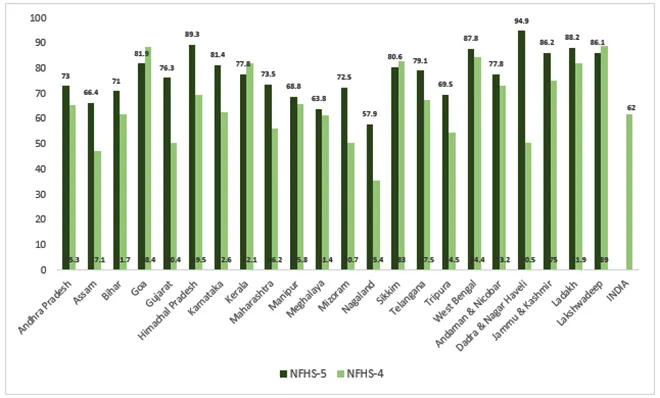
The recent NFHS-5 data (2019-20) from 22 states/UTs indicates an improvement on the full immunisation coverage in children (12-23 months) as indicated in figure 1. Going by the national figures from NFHS-4 (2015-16) the full immunisation rate was 62 percent.
Figure 1: Children 12-23 months fully immunized in 22 states/UTs
A major problem in India and other similarly high-burden countries is the inequality in vaccine administration amongst vulnerable children. Evidence suggest socioeconomic status-based vaccine disparity with the disadvantaged and undeserved groups being left out. Recent reviews show a slight improvement in wealth-related inequality in a few states in India; however, a more targeted approach is needed to overcome it. Vaccine coverage for India has gone up by only 19 percent in the decade from 2006 to 2016, largely attributable to lack of awareness, migrant population that does not have access to healthcare and to vaccination. On other hand, vaccine hesitancy is a challenge for India. there are many factors that contribute to vaccine hesitancy including parents’ literacy, their income, their knowledge on the vaccination schedule and false beliefs. The pandemic has seen the rise of vaccine hesitancy amongst the educated and privileged as well due to a proliferation in misinformation. An analysis of the IMI has found that lack of skills and inadequate time are the key limiting factors on the capabilities of community health workers in providing effective counselling. It suggests for providing clear, accurate information to counter misinformation and myths around vaccination.
In order to address the disruption of routine immunisation by the pandemic, the Indian Academy of Paediatrics has issued recommendations for routine immunisation of COVID-19 suspected and positive children. Immunisation is beneficial and far outweigh the risk of an actual infection as observed during the Ebola outbreak, where the number of deaths due to measles, malaria, and tuberculosis due to disruption of health services far exceeded that from Ebola. According to a benefit–risk analysis of health benefits versus excess risk of SARS-CoV-2 infection in Africa, ‘for every one excess COVID-19 death attributable to SARS-CoV-2 infections acquired during routine vaccination clinic visits, 84 deaths in children could be prevented by sustaining routine childhood immunisation’.
An analysis of the IMI has found that lack of skills and inadequate time are the key limiting factors on the capabilities of community health workers in providing effective counselling.
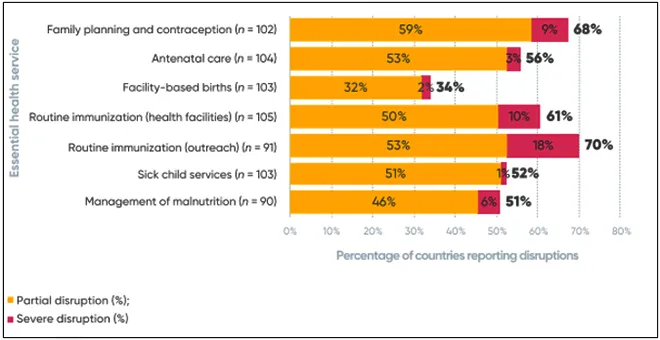
As early as March-April 2020, an alarming 5 million children from across 600,000 villages in India may have lost their chance for routine immunisation. A survey by paediatricians to understand COVID-19 related disruptions to routine vaccination services in India, reported a 50 percent decline in vaccination services with slow recovery. More than 75 percent expressed concern over the gap in vaccination coverage leading to non-COVID morbidity and mortality. Essential health services have been affected across the board as per the WHO’s Pulse survey on continuity of essential health services during the COVID-19 pandemic (figure 2). The most frequently disrupted services include routine immunisation services – outreach services (70 percent) and facility-based services (61 percent).
Figure 2: Percentage of countries reporting disruption in essential health and nutrition services
A narrative review in line with WHO’s guidance document recommends sustaining immunisation programmes, specially focusing on the vulnerable who missed out during the pandemic. India rolled out the IMI 3.0 in February 2021, targeting children and pregnant women who missed out on routine immunization during the pandemic. A review indicates a systematic approach to close the immunisation gap with a prepared health system to address the immunisation challenge and equitable rollout of vaccines.
Improving access to immunisation is critical to achieving the Sustainable Development Goals. There is an urgent need to make efforts to restore the routine immunisation program immediately with all precautionary measures as per WHO guidelines. The Lancet calls for strengthening routine immunisation and outreach to prevent risk of vaccine-preventable disease in children and accelerate progress for a more equitable vaccination coverage. Greater efforts to communicate the benefits of vaccines through health education and counselling, along with immunisation delivery approaches under safe conditions for the health worker, caregiver and the community needs to be adopted. Thus, it is time to invest in immunisation programmes to secure the lives of the future generations.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.





