The prevalence of malnutrition—encompassing both undernutrition and overnutrition—is an important indicator of a country’s health. Those who are either undernourished or are obese underperform in various aspects of life, missing out on opportunities to become productive members of society. India is among those countries in the world with the highest recorded numbers of undernourished. As the country aspires to fulfil its economic and social development goals, malnutrition is one area which requires greater attention. This brief offers an overview of the state of malnutrition in India and documents efforts being made to overcome the problem. It examines India’s performance in key malnutrition indicators, as well as the success, or lack thereof, of various policy measures and programmes initiated over the last few decades. The brief argues that India’s malnutrition challenge can be addressed only when the State governments adopt a comprehensive and coordinated approach and demonstrate better governance; civil society must also respond.
Introduction
Good health benefits not only the individual, but the nation as well. In many countries across the globe, the path to quality health for large proportions of their population is fraught with difficulties. In poor economies, people suffer from various health-related ailments, irrespective of their income level. Though efforts are being made by State and non-State actors to address these health problems, many countries continue to lag in meeting their goals and targets.
The health condition of an individual is determined by a variety of factors – among them, social, economic, dietary, lifestyle, environmental, locational, institutional, and awareness. It is because health is a confluence of these variables that the people who are the worst off are those with low incomes, living in environmentally degraded or remote areas, in developing countries.
Perhaps the most critical for an individual’s health is the foundation built in their early years. If, for instance, a pregnant woman is undernourished, the infant in her womb is similarly not fed properly. Newborns who do not get the desired amount of nutrition may likely not survive. Most recent available estimates show that in some developing countries, including India, nearly half of children under five years of age die each year due to poor nutrition.[1]Those who survive under the same conditions experience serious health disorders at various stages of their life. For the poor, it is highly difficult, if not impossible, to bear the healthcare costs. The middle class and affluent population, meanwhile, show a different trend.[2]A considerable proportion of them lead sedentary lifestyles and consume processed food in excessive quantities. Such unhealthy habits often result in weight gain and an increase in risk of contracting certain diseases.[3]Thus, they get trapped in what health experts refer to as “an abnormal physiological condition called ‘malnutrition’, caused by inadequate, unbalanced or excessive consumption of macronutrients and/or micronutrients”.[4]
This paper begins with a description of the adverse impacts of malnutrition on different population groups in India—newborns, adolescents, and adults. The description is based on a review of all-India and State-level data on stunting, wasting, obesity, and anaemia. The next section examines the policy measures and programmes launched beginning the dawn of an independent India to combat malnutrition. Reference is made to progress achieved with respect to key health and nutrition indicators as well as the concerns expressed by the international community through the UN’s Millennium Development Goals, particularly Goal 1 on eradicating extreme hunger and poverty. This is followed by an explanation of the multiple factors that are responsible for the occurrence of malnutrition, including economic and employment situation, awareness, access to food and safe sanitation, social practices, institutional functioning, experiences in implementation of programmes, and data availability. This section also discusses novel practices underway and offers ideas on interventions needed to overcome the challenges. The concluding section summarises the main points presented in the paper.
Malnutrition in India: A Snapshot
The state of hunger and malnutrition in India is worrying. Statistics compiled by the Food and Agricultural Organisation (FAO) show that while the Sub-Saharan countries of Africa have the highest prevalence of hunger, in absolute terms, India has the highest number (one quarter) of undernourished[5](hungry) people in the world (194.6 million or 15 percent of India’s total population during 2014-16).[6]
Hunger and undernourishment lead to severe problems. Children and youth in this state suffer from numerous nutritional deficiencies which adversely impact their overall health. In India, data for 2015-16[7]show the following:
38 percent of children below five years (urban: 31%, rural: 41%) are stunted (low height for age);
21 percent (urban: 20%, rural: 22%) are wasted (low weight for height);
36 percent (urban: 29%, rural: 38%) are underweight (low weight for age);
2 percent were overweight in 2006[8](above normal weight for height); and
58 percent of children aged between 6 and 59 months (urban: 56%, rural: 59%) are anaemic.[9]
Malnutrition in children under-five also results in nearly half of the 1.3 million deaths occurring in the country each year. Among India’s adolescents, the proportion of overweight and obese was estimated at 11 percent and two percent, respectively, in 2007.[10]Data on anaemia show that 56 percent of young girls and 30 percent of young boys in the age group of 15-19 years are anaemic.[11]
The undesirable impacts of malnutrition are significant in adults, too. For example, the Body Mass Index (BMI or the ratio of weight-for-height) of a sizeable proportion of women (23 percent) and men (20 percent) in the age group 15-49 is found to be falling below the norm.[12]Evidence exist that people with low BMI are more susceptible to tuberculosis than those who have normal BMI; thus there is an immediate need to address the problem of undernutrition.[13]Further, anaemia is prevalent in women (53 percent) and men (23 percent) in the 15-49 age group,[14]indicating lack of iron, which is among the most prevalent manifestations of lack of proper nutrition. Meanwhile, about 21 percent of women and 19 percent of men in the same age group are either overweight or obese.[15]Siddiqui and Donato refer to a dramatic increase in the prevalence of obesity and its consequent impact on the burden of non-communicable diseases (NCD) such as diabetes and cardiovascular disease.[16]
Table 1: Nutrition Status of Indian Population, by State/UT, 2015-16
State / Union Territory
Children (under 5 years)
Adults (15 – 49 years)
BMI below normal
Overweight or Obese
Anaemic
Stunted
Wasted
Underweight
Anaemic
(6-59 months)
Women
Men
Women
Men
Women
Men
A & N Islands-UT
23.3
18.9
21.6
49.0
13.1
8.7
31.8
38.2
65.7
30.8
Andhra Pradesh
31.4
17.2
31.9
58.6
17.6
14.8
33.2
33.5
60.0
26.9
Arunachal Pra.
29.4
17.3
19.5
50.7
8.5
8.3
18.8
20.6
40.3
16.9
Assam
36.4
17.0
29.8
35.7
25.7
20.7
13.2
12.9
46.0
25.4
Bihar
48.3
20.8
43.9
63.5
30.4
25.4
11.7
12.6
60.3
32.2
Chandigarh-UT
28.7
10.9
24.5
73.1
13.3
21.7
41.5
32.0
75.9
19.3
Chhattisgarh
37.6
23.1
37.7
41.6
26.7
24.1
11.9
10.2
47.0
22.2
Daman & Diu-UT
23.4
24.1
26.7
73.8
12.9
12.0
31.6
30.7
58.9
23.6
D & N Haveli-UT
41.7
27.6
38.9
84.6
28.5
19.7
19.2
22.9
79.5
30.7
Delhi NCT-UT
32.3
17.1
27.0
62.6
12.8
17.7
34.9
24.6
52.5
21.6
Goa
20.1
21.9
23.8
48.3
14.7
10.8
33.5
32.6
31.3
11.0
Gujarat
38.5
26.4
39.3
62.6
27.2
24.7
23.7
19.7
54.9
21.7
Haryana
34.0
21.2
29.4
71.7
15.8
11.3
21.0
20.0
62.7
20.9
Himachal Pra.
26.3
13.7
21.2
53.7
16.2
18.0
28.6
22.0
53.4
20.1
Jammu & Kashm.
27.4
12.1
16.6
43.3
12.1
11.5
29.1
20.5
40.3
15.1
Jharkhand
45.3
29.0
47.8
69.9
31.5
23.8
10.3
11.1
65.2
29.9
Karnataka
36.2
26.1
35.2
60.9
20.7
16.5
23.3
22.1
44.8
18.2
Kerala
19.7
15.7
16.1
35.6
9.7
8.5
32.4
28.5
34.2
11.3
Lakshadweep-UT
27.0
13.8
23.4
51.9
12.5
7.4
41.4
24.6
45.7
10.7
Madhya Pradesh
42.0
25.8
42.8
68.9
28.3
28.4
13.6
10.9
52.5
25.5
Maharashtra
34.4
25.6
36.0
53.8
23.5
19.1
23.4
23.8
48.0
17.6
Manipur
28.9
6.8
13.8
23.9
8.8
11.1
26.0
19.8
26.4
9.6
Meghalaya
43.8
15.3
29.0
48.0
12.1
11.6
12.2
10.1
56.2
32.4
Mizoram
28.0
6.1
11.9
17.7
8.3
7.2
21.1
21.0
22.5
9.6
Nagaland
28.6
11.2
16.8
21.6
12.2
11.5
16.2
14.0
23.9
10.1
Odisha
34.1
20.4
34.4
44.6
26.4
19.5
16.5
17.2
51.0
28.4
Punjab
25.7
15.6
21.6
56.6
11.7
10.9
31.3
27.8
53.5
25.9
Puducherry-UT
23.7
23.6
22.0
44.9
11.3
10.2
36.7
37.1
52.4
15.9
Rajasthan
39.1
23.0
36.7
60.3
27.0
22.7
14.1
13.2
46.8
17.2
Sikkim
29.6
14.2
14.2
55.1
6.4
2.4
26.7
34.8
34.9
15.7
Tamil Nadu
27.1
19.7
23.8
50.7
14.6
12.4
30.9
28.2
55.1
20.4
Telangana
28.1
18.0
28.5
60.7
23.1
21.4
28.1
24.2
56.7
15.4
Tripura
24.3
16.8
24.1
48.3
18.9
15.7
16.0
15.9
54.5
24.7
Uttarakhand
33.5
19.5
26.6
59.8
18.4
16.1
20.4
17.7
45.2
15.5
Uttar Pradesh
46.3
17.9
39.5
63.2
25.3
25.9
16.5
12.5
52.4
23.7
West Bengal
32.5
20.3
31.5
54.2
21.3
19.9
19.9
14.2
62.5
30.3
India
38.4
21.0
35.7
58.4
22.9
20.2
20.7
18.6
53.0
22.7
Source:Ministry of Health and Family Welfare. NFHS-4. 2015-16. All-India and State/UT Fact Sheets. Mumbai: IIPS.
Notes: (i) All figures in percent; (ii) shades denote the following:
States/UTs recording highest percentages.
States recording lowest percentages.
Nutrition data generated from the fourth National Family Health Survey (NFHS-4) conducted in 2015-16 are now available for all Indian States/Union Territories. The following inferences may be drawn from the data on nutritional status presented in Table 1:
The nutritional status of children under five years is critical in the States/UTs of Bihar, Jharkhand, Uttar Pradesh, and Dadra and Nagar Haveli; Kerala and Mizoram are faring better.
BMI below normal is most evident in Bihar, Jharkhand, Madhya Pradesh, and Uttar Pradesh; status is better in Sikkim.
The incidence of overweight or obesity is highest in Chandigarh, Lakshadweep, Andaman and Nicobar Islands, and Puducherry; the situation is better in Bihar and Meghalaya.
Anaemia is most prevalent in Chandigarh, Dadra & Nagar Haveli, Bihar and Meghalaya; it is lowest in Manipur and Mizoram.
The nutrition profile of Indian States/UTs thus presents wide variations among the different regions. Generally, data and literature reveal that the condition of poor families (children, women and men), with respect to the intake of calories, proteins, and micro-nutrients, is inferior in rural areas, poorer States, and in city slums. On the other hand, the middle- and high-income populations, concentrated in Indian cities, are becoming more susceptible to so-called ‘lifestyle diseases’ and ‘binge-eating disorders’ caused by increased availability of processed and sugary foods and drinks.[17]
Policy and Programme Interventions
India’s Nutrition Policy of 1993 was shaped on the basis of a detailed understanding of the factors responsible for the occurrence of malnutrition.[18]The policy called for the adoption of a multi-sectoral approach and the implementation of a wide range of measures to achieve the goal of optimum nutrition for all. Subsequently, numerous plans, programmes and missions were launched on various occasions (Box 1).
Box 1: Government Policy Interventions and Programmes to Combat Malnutrition
Direct Policy Measures
Plans, Programmes and Missions
Expand the safety net through ICDS to cover all vulnerable groups (children, adolescent girls, mothers, expectant women)
Fortify essential foods with appropriate nutrients (e.g., salt with iodine and/or iron)
Popularise low cost nutritious food
Control micro-nutrient deficiencies amongst vulnerable groups
Indirect Policy Measures
Ensure food security through increased production of food grains
Improve dietary pattern by promoting production and increasing per capita availability of nutritionally rich food
Effecting income transfers (improve purchasing power of landless, rural and urban poor; expand and improve public distribution system)
Other: Implement land reforms (tenure, ceiling laws) to reduce vulnerability of poor; increase health and immunisation facilities, and nutrition knowledge; prevent food adulteration; monitor nutrition programmes and strengthen nutrition surveillance; community participation
Mid-day Meal Programme, 1962-63
Goitre Control Programme, 1962 (now known as National Iodine Deficiency Disorders Control Programme)
Special Nutrition Programme, 1970-71
Balwadi Nutrition Programme, 1970-71
Nutritional Anaemia Prophylaxis Programme, 1970
Prophylaxis Programme against Blindness due to Vitamin A Deficiency, 1970
Integrated Child Development Services (ICDS), 1975
National Diarrhoeal Diseases Control Programme, 1981
National Health Mission, 2013 (subsumes former Rural & Urban Health Missions)
National Iron+ Initiative, 2013
Promotion of Infant & Young Child Feeding Practices Guidelines, 2013
Weekly Iron & Folic Acid Supplementation, 2015
National Deworming Day, 2015
Establishment of: Nutritional Rehabilitation Centres; Village Health Sanitation & Nutrition Committee
Bi-annual Vitamin-A Supplementation
Village Health & Nutrition Days (at Anganwadi centers)
Source:National Nutrition Policy, 1993; Ministry of Health and Family Welfare.Annual Report 2015-16. Chapter 3 – Maternal and Adolescent Healthcare p. 27-31; Chapter 4 – Child Health Programme, p. 39. New Delhi: Department of Health and Family Welfare; The Indian Express, 30 December 2015,Op.cit.
Note: Year mentioned against the name of a programme denotes the year in which the programme was launched in the country for the first time.
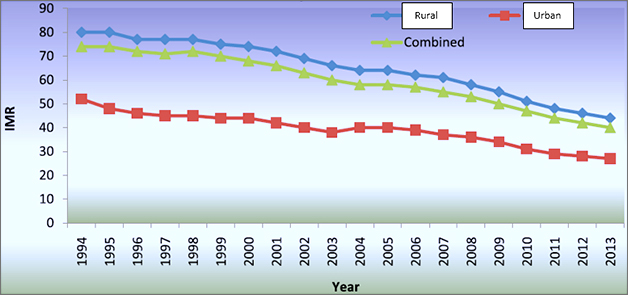
Figure 1: Infant Mortality Rate in India, 1994-2013
Figure source:CBHI. National Health Profile, 2015, p. 19;Data source:Registrar General of India. SRS Bulletin, September 2013;Note:IMR in per 1,000 live births.
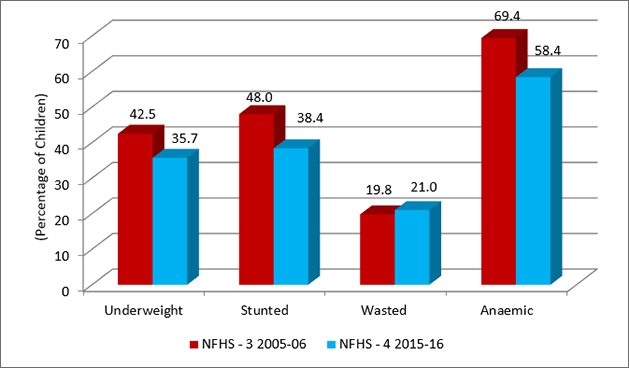
Figure 2: Nutrition and Anaemia Status of Children in India
Source:NFHS – 4, 2015-16; Note: Data on anaemia pertain to children aged 6-59 months.
The policy and programme measures initiated in the health sector address various aspects of nutrition and are helping to mitigate the problem. This is evident in the following patterns of decline in some of the country’s key health variables: (i) proportion of undernourished persons in the total population from 24 percent in 1990-92 to 15 percent in 2014-16;[19](ii) maternal mortality ratio from 398 in 1997-98 to 167 per 100,000 live births in 2011-13;[20](iii) infant mortality rate from 80 in 1991 to 41 per 1,000 live births in 2015-16;[21](iv) under-five mortality rate from 115 in 1991 to 50 per 1,000 live births in 2015-16;[22](v) percentage of children underweight, stunted, and anaemic[23](Figures 1 and 2).
The UN has established international development goals to monitor the progress on numerous social, economic and environmental inequalities. With respect to MDG 1 (i.e., eradicate extreme poverty and hunger), the UN had observed that India was still far behind (slow or almost off-track) the 2015 target (No. 1. C) of halving, between 1990 and 2015, the proportion of people who suffer from hunger, and the government must take immediate actions “to ensure India accelerates progress on hunger”.[24]When the goal was formulated in 1990, 53.5 percent of all Indian children were malnourished. By 2015, malnutrition declined to 40 percent. This change was noted from NFHS estimates particularly in the proportion of underweight children below three years. Thus, the target of halving the proportion of malnourished children to 26 percent (which is one-half of the proportion recorded in 1990) was not achieved.[25],[26] Following the end of the MDG period in 2015, 17 Sustainable Development Goals (SDG) were announced by the UN in 2016 for the period ending 2030. SDG 2 calls to “end hunger, achieve food security and improved nutrition, and promote sustainable agriculture”.
The current Union Health Minister, JP Nadda, has also urged for finding “solutions for accelerating action at the State level”.[27]There is also a discussion on formulating a National Nutrition Strategy by the present government for the benefit of poorly performing States and districts in the country.[28]
A Web of Factors Causing Malnutrition
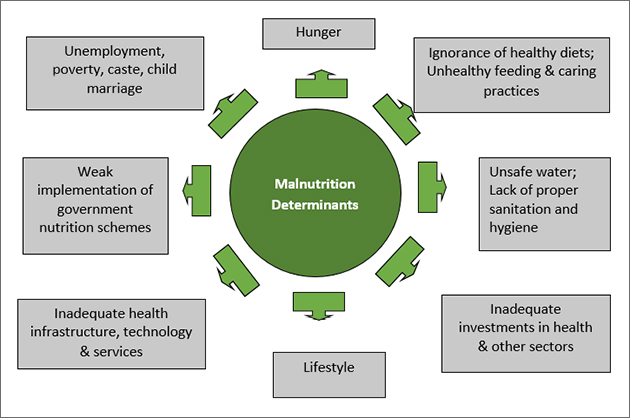
As there are a multiplicity of factors that ensure that every single human being receives sufficient nutrition, similarly, there are manifold variables that contribute to the occurrence of malnutrition in India (Figure 3).[29]
Figure 3: Common Reasons for Prevalence of Malnutrition
Source:Author’s own.
It is clear from Figure 3 that economics plays a crucial role in healthcare. After all, families need money to be able to look after their daily needs, including a healthy diet, safe water, and sanitary living conditions. In India, there is a highly significant problem of uncertainty of income[30]among the rural population (especially agricultural labourers), marginalised groups, and the informal sector. Poverty data for 2013 compiled by the World Bank reveal that as much as 30 percent (224 million) of the country’s population live below the international poverty line of less than $ 1.90-a-day.[31]India’s own poverty estimates lack accuracy due to methodological deficiencies, and more studies are needed to examine the relationship between the people’s economic condition and the incidence of malnutrition in villages and towns. The country’s Labour Bureau also recorded a high unemployment rate in India of five percent in 2015-16 (8.7 percent for women, 4.3 percent for men, 5.1 percent for rural sector, and 4.9 percent for urban sector).[32]
Besides income, also absent are sufficient health and nutrition awareness among the people (about wholesome, balanced and natural diets; healthy child-feeding and caring practices).[33]It is an imperative therefore to run an effective nutrition communication campaign (in schools, public places, print and social media) that would help children and communities, regardless of their income and education levels, in understanding how they should respond to their nutritional needs.
People’s access to sufficient and nutritious food is equally important. India’s situation in this regard has been noted as “serious” by the International Food Policy Research Institute (IFPRI). IFPRI’s Global Hunger Index (GHI) shows India ranked 97 among 118 countries on hunger in 2016.
One effort to address the hunger (and nutrition) challenge is the enactment of the National Food Security Act. Put into effect in 2013, the law aims to ensure greater access to adequate quantity of quality food at affordable prices. Up to 75 percent of eligible rural and 50 percent of eligible urban population as identified by States/UTs are entitled to receive food grains (five kg per person per month of rice, wheat, coarse grains at subsidised prices of INR 3/2/1 per kg, respectively) under the Targeted Public Distribution System (PDS) launched in June 1997. Besides ensuring access to food grains, the Act also provides for monetary maternity benefits, and the establishment of a grievance redressal mechanism to ensure compliance by State/District government functionaries.
A 2015 survey by Swaraj Abhiyan, a political organisation, reveals unsatisfactory progress in the implementation of the Act.[34]Data samples collected from Uttar Pradesh show that at places experiencing famine-like conditions, barely half of the poor families had eaten any pulses in the 30 days preceding the survey. According to Drèze, such problems will continue unless greater efforts are made to strengthen the existing initiatives (such as the Public Distribution System, Mid-day Meal Scheme, ICDS, Village and Child Development Centres).[35]Loss of food grains in FCI warehouses (due to rotting and theft) is an equally important reason for the lack of adequate access.[36]
There is also the Integrated Child Development Services (ICDS) Scheme that has benefitted India’s over 100 million persons including children, pregnant women and lactating mothers.[37]However, problems are being observed in ensuring supply of quality food, and its uniform distribution.[38],[39] Anganwadi centres[40]were established under ICDS to provide basic healthcare education and services across the country. Many workers are unable to play an effective role in attending to the problem of malnutrition because of low wages and inadequate training.[41]Organisation of regular orientation programmes, exposing workers to new techniques available for tracking the growth of every child, and supporting them in the implementation of schemes would be useful in improving the country’s nutrition situation.
Other examples exist to illustrate the failure of service delivery. The Village Child Development Centres (VCDC), for instance, were set up in 36 districts of Maharashtra in 2016 with the support of the Central government to provide malnourished children with medical care and nutritious meals for one month. However, most of the centres have been found to be non-functional due to the absence of funds. In view of the risk to about 78,925 severely malnourished children in the State, local non-government organisations want the State government to step in and take responsibility for funding the VCDCs.[42]
Compounding the economic and political factors that abet malnutrition are social and cultural challenges that tend to defeat the very purpose of a nutrition programme. To begin with, India’s massive population comprises such diverse community groups, of whom over 200 million (16.6 percent) are classified as ‘scheduled castes’. A plan, for instance (namedHausla Poshan Yojana) to provide nutritious food to pregnant women and malnourished children in Uttar Pradesh failed to even take off because there were supposed women beneficiaries who refused to consume the food prepared by Anganwadi workers belonging to the scheduled caste community,[43]who have been historically regarded as untouchables by the upper castes. Further, Census data for 2011 show high incidence of child marriage in India (30 percent of all marriages). According to research published in theBritish Medical Journal, “infants born to child brides in India (married before the age of 18) have a higher risk of malnutrition”.[44]As the mothers of these children are themselves children, and themselves undernourished, these infants are simply being born into the cycle of undernourishment.
To improve nutritional content in food products, steps are being taken towards universal food fortification.[45]A proposed policy would provide for adding essential vitamins and minerals (iron, folic acid, vitamin, iodine) to food items (rice, wheat flour, salt, edible oil, milk) sold in markets. The Food Safety and Standards Authority of India (FSSAI) has set nutritional benchmarks to ensure that manufacturers responsible for fortifying food add desirable levels of micronutrients to the food items. Valuable lessons in this regard have been learnt from practices followed in the Gajapati district of Odisha where training was given to school staff engaged in preparing mid-day meals for schoolchildren so that they are able to fortify the rice with iron for increasing its nutritional value. About 1,449 schools in the district have been covered under the programme, and the Central government is interested in extending this initiative to other parts of the country as well.[46]According to the Department of Biotechnology (DBT), “clinical studies have substantiated that regular feeding for one year increases iron store and decreases anaemia in school going children”. Care is however needed in ensuring that people do not consume iron beyond the required amounts, as some studies suggest a direct link between iron and diabetes.[47]
Needless to say, adequate funds are needed for the successful implementation of any nutrition scheme. In the case of India, with respect to centrally supported schemes such as ICDS, data show that the budgetary allocations have decreased over time. Between 2014-15 and 2015-16, financial allocations were halved from INR 166 billion to INR 83 billion. More recently, while the allocations have increased in absolute terms, the annual rate of change is down to 12.76 percent (Table 2). The national government maintains that the State governments must play a more pro-active role in combating malnutrition and themselves generate funds for this purpose.
Table 2: Central Budgetary Allocations for Integrated Child Development Services Scheme
Financial Year
Budgetary Allocations
Annual Change
(in INR billions)
(percent)
2013-14
163.12
–
2014-15
165.61
1.53
2015-16
83.36
– 49.66
2016-17
148.50
78.14
2017-18
167.45
12.76
Source:Ministry of Women and Child Development. Press Information Bureau releases, 19 March 2015 and 1 February 2017.
Article 47 of the Indian Constitution provides that it is the “duty of the State to raise the level of nutrition and the standard of living and to improve public health”. Compliance with this provision is seen in the form of nutrition missions launched by some State governments.
Maharashtra’s nutrition mission (2005), for instance, aims to reduce malnutrition in all its forms. The mission strategy includes the following aspects: deliver evidence-based interventions; focus on adolescent girls’ nutrition, education and empowerment; combine facility, outreach and community-based interventions to bring services and support closer to the people; and monitor pregnancy weight gain at every ante-natal care visit. For this purpose, a multi-sectoral action plan is in use.[48]Today, the mission is seen as a model because it has contributed to encouraging improvements in the people’s nutritional status.[49]
In Madhya Pradesh (2010), meanwhile, INR 500 million were allocated under the mission, and the following steps were taken: preparation of district-level action plans; initiation of pilot projects; monitoring and evaluation of progress indices; and provision of meals to pregnant women at Anganwadi centres.[50]
Similar initiatives have been undertaken in Karnataka (2010), Gujarat (2012), and Uttar Pradesh (2014). In 2015 a mission was also launched, with technical support from UNICEF, in Jharkhand where the situation of malnutrition is critical (see Table 1).[51]Some of the mission’s goals and features are the following:
Make the State malnutrition-free within 10 years;
Create a database of pregnant mothers;
Modernise Anganwadis through the use of corporate social responsibility funds;
Improve nutrition awareness of communities;
Foster inter-sectoral collaboration for nutrition action among departments.
Further, nutrition interventions and tracking progress cannot be done without sufficient information and reliable, updated data, and the operationalisation of a national nutrition surveillance system. Thus, there exists the need to collect and maintain real-time data on various nutrition indicators using ICT and GIS.
Lack of sanitation is also an important determinant of malnutrition. In India, open defecation remains a severe problem as a significant proportion of the population either do not give importance to the use of clean toilets and therefore do not build them, or are in no position to build within their living spaces due to income or space issues. This situation is observed mainly in the rural areas as well as among the city’s slum dwellers. Data from the National Sample Survey conducted in May-June 2015 show that more than half of India’s rural population (52.1 percent) defecates in the open, while the prevalence among the urban proportion stands at 7.5 percent.[52]Poor sanitary conditions caused by open-defecation and other issues, in turn, lead to the incidence of diarrhoeal diseases; these diseases make children susceptible to stunting.[53]The government aims to make India open defecation-free by 2019, and accordingly, work is underway on the construction of household, community, public toilets under the Swachh Bharat Mission. Yet again, the implementation and maintenance is weak, as observed from the slow progress in meeting the targets, and the existence of several newly constructed but non-functional toilets.[54]
Besides the above-mentioned government interventions, judicial and civil society activism is making inroads in bringing down India’s malnutrition rates.[55]For example, the Right to Food Campaign (launched in March 2014), which is an informal network of individuals and organisations, is the result of public interest litigation. Under the campaign, organised efforts are made to persuade State governments to attend to the most pressing demands of society, including proper nutrition.
Conclusion
An overview of the malnutrition situation in India presented in this paper has shown that a sizeable proportion of the country’s population are malnourished and anaemic, and for this, numerous factors are responsible. Some of these factors directly cause malnutrition among people, whereas many others affect indirectly. Significant among these are poverty; unemployment; ignorance and lack of education; unhealthy lifestyle; lack of access to nutritious food, safe water, sanitation and hygiene; non-availability of reliable and timely data, and sufficient funds; and unimpressive performance by the government in the implementation of schemes.
Many of the reasons for the occurrence of malnutrition, as well as the solutions to overcome the challenge, are known. Attention, however, needs to be paid to understanding what prevents the nation from achieving its goals related to nutrition. Undoubtedly, the agencies of State governments have to adopt a comprehensive and coordinated multi-sectoral approach which is formulated by taking into account the varied nature of local-level challenges. They have to demonstrate better governance, too. For its part, civil society must respond in a responsible manner. In particular, attention needs to be paid on building neighbourhood health and nutrition profiles and carrying out interventions based on identified needs.
Endnotes
[1]UNICEF, WHO, World Bank Joint Child Malnutrition dataset, updated May 2017. Available from: https://data.unicef.org/topic/nutrition/malnutrition/
[2]Giri, Rujuta and Vanisha S. Nambiar. ‘Dietary habits, parental history and dual burden of malnutrition among affluent school going children’,International Journal of Current Research, 8 (5): 31446-31451, May 2016.
[3]Bierly, Allison. ‘Certain foods linked to long-term weight gain’. National Institutes of Health, 11 July 2011.
[4]FAO, IFAD and WFP.The State of Food Insecurity in the World. Rome: FAO, 2015.
[5]Undernourishment is “a state, lasting for at least one year, of inability to acquire enough food, defined as a level of food intake insufficient to meet dietary energy requirements” (FAO. Op. cit, p. 53).
[6]FAO, IFAD and WFP.Ibid; International Business Times. ‘India has most number of hungry people in the world: Report’, 31 May 2016.
[7]Data on different nutrition indicators are generated through National Family Health Surveys (NFHS). So far, four rounds of surveys have been conducted, i.e., NFHS-1 (1992-93), NFHS-2 (1998-99), NFHS-3 (2005-06) and NFHS-4 (2015-16).
[8]IFPRI.Global Nutrition Report, Nutrition Country Profile – India, 2015: data beyond 2006 are not available.
[9]NFHS – 4. 2015-16. Anaemia implies deficiency of red cells or of haemoglobin in blood, which causes weakness.
[10]IFPRI. Op. cit., data beyond 2007 are not available.
[11]The Indian Express. ‘Health ministry kicks off programme to reduce anaemia among adolescents’, 30 December 2015.
[12]NFHS – 4. 2015-16; According to the WHO definition, a BMI of less than 18.5 kg. per square meter indicates severe thinness.
[13]Bhargava, Anurag. ‘Undernutrition, nutritionally acquired immunodeficiency, and tuberculosis control’. Editorials,British Medical Journal, October 2016.
[16]Siddiqui, Md. Zakaria and Ronald Donato. ‘Overweight and obesity in India: Policy issues from an exploratory multi-level analysis’.Health Policy and Planning, 31 (5): 582-591, June 2016.
[18]Ministry of Human Resource Development.National Nutrition Policy, p. 3-6. New Delhi: Department of Women and Child Development, 1993.
[19]FAO, IFAD and WFP.The State of Food Insecurity in the World,p. 46, Op. cit.
[20]Ministry of Health and Family Welfare.Annual Report 2015-16, Chapter 3 – Maternal and Adolescent Healthcare, p. 26. New Delhi: Department of Health and Family Welfare.
[21]NIMS, ICMR and UNICEF.Infant and Child Mortality in India – Levels, Trends and Determinants, Fact Sheet; Ministry of Health and Family Welfare.Annual Report 2015-16, Chapter 4 – Child Health Programme, p. 37. New Delhi: Department of Health and Family Welfare; NFHS – 4.
[23]NFHS – 4; The India Health Report on Nutrition (PHFI, 2015) observes “stunting, wasting and underweight rates of India’s children have declined, but still exceed levels observed in countries at similar income levels”.
[24]UN.India and the MDGs – Towards a Sustainable Future for All. UN ESCAP, 2015.
[25]UNDP, 2015. Available from http://www.in.undp.org/content/india/en/home/post-2015/mdgoverview.html
[26]MoSPI.Statistical Year Book India 2016, Chapter 45 – Millennium Development Goals.
[27]The Times of India. ‘Malnutrition down, but not enough’, 11 December 2015.
[28]The Times of India. ‘National nutrition strategy will be out soon; focus areas to be shortlisted’, 6 November 2015.
[29]For writing this section of the paper, the author has also reviewed the UNICEF conceptual framework which describes three levels of causes of undernutrition. Available from: https://www.unicef.org/nutrition/training/2.5/4.html
[30]IDFC.India Rural Development Report 2013-14. Delhi: Orient BlackSwan.
[31]Business Today. ‘India has highest number of people living below poverty line: World Bank’, 3 October 2016.
[32]The Indian Express. ‘India’s unemployment rate highest in 5 years in 2015-16’, 29 September 2016.
[33]Planning Commission.Addressing India’s Nutrition Challenges, Report of the Multistakeholder Retreat, p. 25, 7-8 August 2010.
[34]The Times of India. ‘Man made starvation’, by Jean Drèze, 21 December 2015.
[36]The Times of India. ‘Grains rotting with FCI could have fed 8L for a year’, 2 May 2016.
[37]Human Rights Council. ‘Third Universal Periodic Review of India’, p. 17, 18 January 2017.
[38]Press Information Bureau. ‘Bad quality food supply for Aanganwadis’, 7 August 2013.
[39]The Pioneer. ‘Thumbs down to packaged food under ICDS’, 22 February 2015.
[40]‘Anganwadi’ is a Hindi word which means ‘courtyard shelter’. Anganwadi centres are run by anganwadi workers, “ladies selected from the local community, who work as agents of social change, mobilising community support for better care of young children, girls and women”. They are paid a monthly honoraria as decided by the government. Further details available from: http://icds-wcd.nic.in/icds/icds.aspx
[41]Tripathi M., et al. ‘Perceived responsibilities and operational difficulties of anganwadi workers at a coastal south Indian city’,Medical Journal, D.Y. Patil University, Vol. 7, Issue 4, pp. 468-472, 2014.
[42]The Times of India. ‘No sign of Rs. 213 cr. to tackle child malnutrition in Maharashtra’, 20 October 2016.
[43]The Times of India. ‘Nutrition plan: Moms-to-be refuse Dalit-served food in UP’, 5 August 2016.
[44]Raj, Anita, Niranjan Saggurti, Michael Winter, Alan Labonte, Michele R. Decker, Donta Balaiah, Jay G. Silverman. ‘The effect of maternal child marriage on morbidity and mortality of children under 5 in India: cross sectional study of a nationally representative sample’. BMJ, 340 (jan21 1), 2010.
[45]Ministry of Women and Child Development. ‘Universal Food Fortification’, Press Information Bureau, 5 August 2016.
[46]Rice-fortification was first launched in Odisha by the UN (under their World Food Programme).
[47]Simcox, Judith A. and Donald A. McClain. ‘Iron and Diabetes Risk’,Cell Metabolism, 17 (3): 329-341, 5 March 2013.
[48]Rajmata Jijau Mother-Child Health and Nutrition Mission – Government of Maharashtra. Available from: http://www.mahnm.in/about
[49]Krishna, Vandana. ‘The Maharashtra nutrition mission’.Seminar, No. 681, May 2016.
[50]Government of Madhya Pradesh, Women and Child Development Department. ‘Atal Bihari Bajpai Child Health and Nutrition Mission’. Available from http://www.mpwcd.nic.in/web/wcd/sc-ic-abm
[51]UNICEF. ‘Jharkhand Nutrition Mission Launched’, 13 November 2015, Available from http://unicef.in/PressReleases/400/Jharkhand-Nutrition-Mission-Launched-
[52]National Sample Survey Office.Swachhta Status Report 2016. Ministry of Statistics and Programme Implementation.
[53]UNICEF.The Impact of Poor Sanitation on Nutrition, Policy Brief. London: SHARE Research Consortium in collaboration with the WASH and Nutrition Sections of UNICEF India, 2015; Spears, Dean. ‘The nutritional value of toilets: How much international variation in child height can sanitation explain?’, Working paper. Delhi: Delhi School of Economics, June 2013.
[54]The Hindu. ‘Most of rural India still opts for open defecation: NSS Report’, 18 September 2016.
[55]Mohmand, Shandana Khan. ‘Policies without politics: Analysing nutrition governance in India’. Institute of Development Studies, February 2012.
The views expressed above belong to the author(s). ORF research and analyses now available on Telegram! Click here to access our curated content — blogs, longforms and interviews.

 PDF Download
PDF Download